Depth of flap elevation
Depth of flap elevation
The depth of flap elevation impacts the size and perfusion pressure of the vessels within the pedicle. Deeper elevation planes incorporate vessels with larger diameters and greater perfusion pressures. The plane of flap elevation differs by anatomic location, and appropriate selection of undermining planes balances maximizing the blood supply with protection of critical anatomic structures (especially branches of the facial motor nerve). Most transposition flaps are elevated at the junction of the subdermal fat and fascia (Fig. 23-10). Routine exceptions include flaps on the midline nose and forehead, which are usually elevated deep to the muscles of facial expression, and those on the scalp, which are elevated deep to the galea aponeurotica (Fig. 23-11).
The width of the flap pedicle A narrow vascular pedicle compromises the blood supply to the flap. Factors influencing the pedicle width include the flap takeoff point and angle from the defect, the location of the standing cone at the pedicle base, and the number of lobes of the flap (e.g., bilobed versus trilobed). Distal takeoff points result in a narrower pedicle than a
proximal takeoff point (Fig. 23-12). The takeoff angle is the angle created between the first limb of the rhombic flap and the primary defect (Fig. 23-13A). As the takeoff angle becomes more acute, the width of the flap pedicle increases (Fig. 23-13B). However, more acute takeoff angles usually require greater secondary motion around the primary defect for wound closure. As noted above, as the arc of flap rotation increases, the standing cone encroaches further into the vascular pedicle of the flap. Finally, as the number of lobes increases, the width of the flap pedicle is enlarged, increasing flap vascularity (Fig. 23-14).
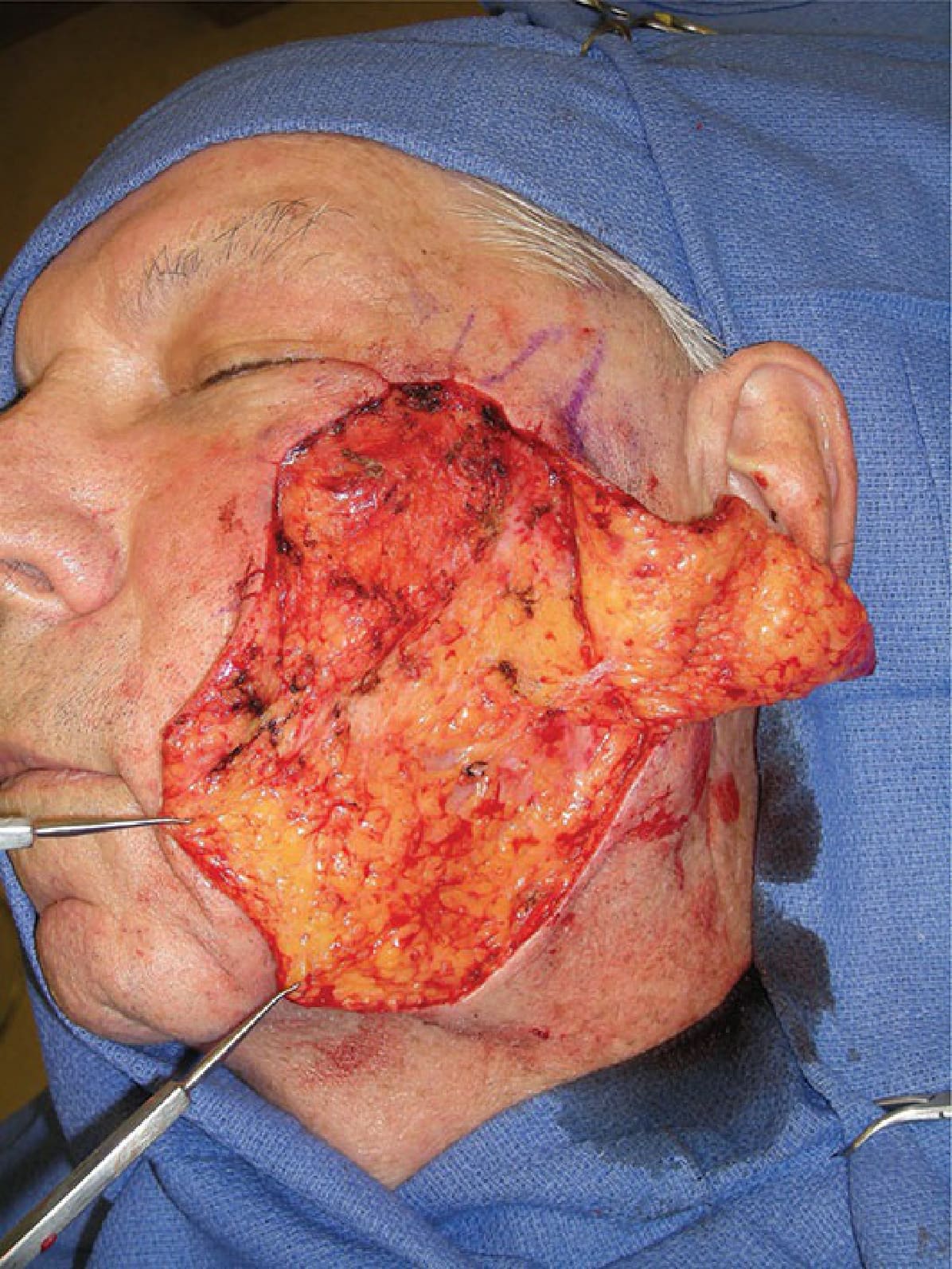
Figure 23-10. Transposition flap elevated underneath the subdermal fat, which consists of smaller, tightly packed lobules. Note that the plane of undermining is above the larger lobules of the buccal fat pad.

Figure 23-11. Transposition flaps on the nose are elevated deep to the muscular layer, above the perichondrium or periosteum.
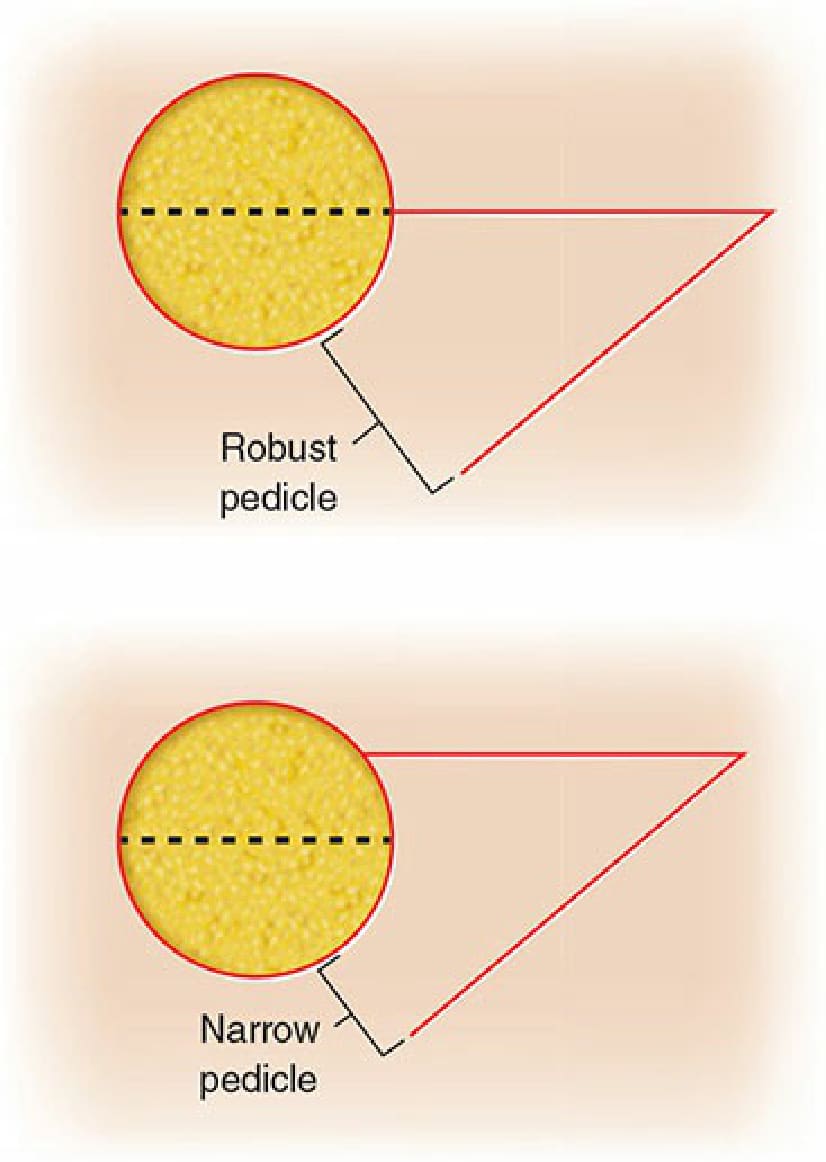
Figure 23-12. Compared to flaps with a takeoff at the midpoint of the defect (top), flaps with distal takeoff points result in a narrower vascular pedicle, which may compromise blood supply (bottom).
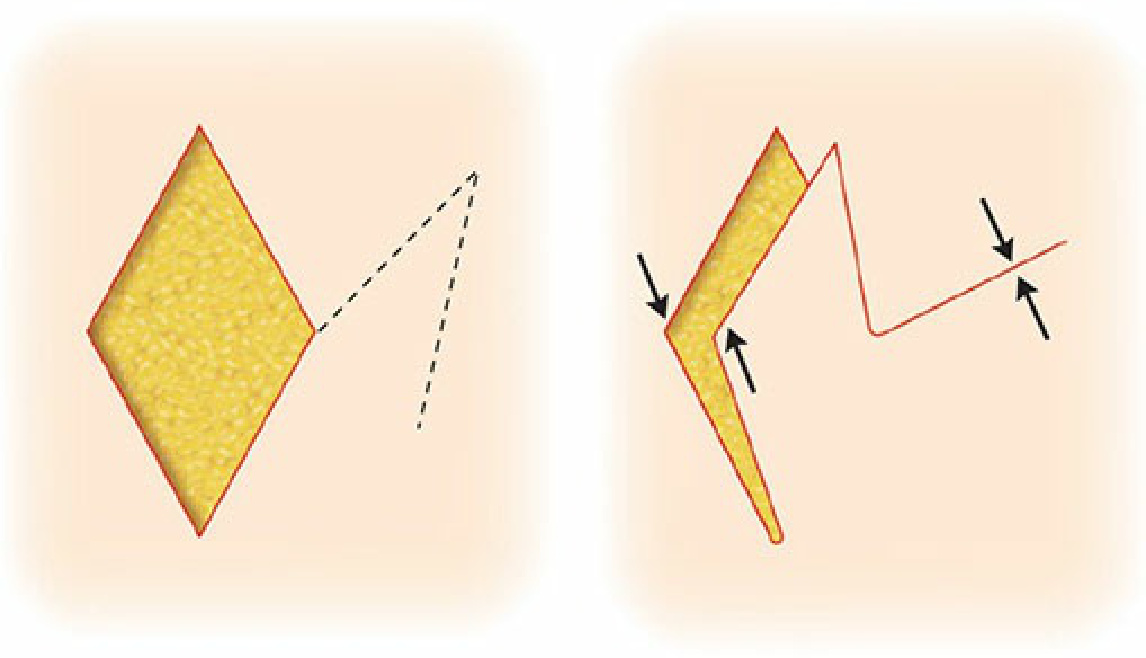
Figure 23-13. Closure of the donor site of a flap with an acute takeoff angle widens the defect, increasing the sharing of tension at the recipient site. Conversely, flaps that take off at a right angle to the defect require less secondary motion.

Figure 23-14. Bilobed flap design for a defect on the distal nose. The standing cone has a slight vertical orientation to avoid alar elevation. Note the narrow and tenuous vascular pedicle (bracket). Closure of the tertiary defect (green arrows) would distort the alar free margins. Converting from bilobed to trilobed flap (B) results in a wider, more robust vascular pedicle (bracket) and creates a terminal donor site that is vertically oriented to minimize alar distortion located at more favorable position within a generous tissue reservoir that facilitates side-to-side closure (green arrows).