Tension vectors
Tension vectors
Transposition flaps reorient and displace tension vectors to adjacent tissue reservoirs, thereby preserving the position of free margins and restoring contour at the primary defect. In general, tension is transferred from the primary defect to the terminal donor site or lobe (i.e., the secondary lobe of a bilobed flap and the tertiary lobe of a trilobed flap; Fig. 23-4). Closing the terminal donor site should allow rotation of the flap into the primary defect with minimal tension (Fig. 23-5). If tension at the primary defect is still excessive, strategically placed tacking sutures can anchor flaps to immobile structures and minimize tension across the dermal sutures (Fig. 23-6). On the central face, tacking the undersurface of the flap to the origin of the zygomaticus major muscle, the inferior orbital rim, or the medial canthal tendon can prevent lower eyelid ectropion, and tacking sutures to the pyriform aperture can mitigate the risk of alar margin distortion.
These tacking sutures also recreate contour when transposition flaps drape over concavities, such as the alar groove or nasal facial sulcus.
Pivotal restraint and flap shortening with increased angle of rotation
Visualizing a rhombic flap as a rotation flap with a large backcut helps illustrate the consequence of pivotal restraint on flap movement (Fig. 23-7). The fixed base at the pedicle tethers the flap and serves as a pivot point as the flap is rotated toward the primary defect. The pivot points for a rhombic flap are shown in Figure 23-8. As the arc of rotation increases, pivotal restraint increasingly restricts and shortens the flap length.1 If the shortened flap does not have enough surface area to cover the defect, the consequent secondary motion of the recipient tissue will increase tension at the primary defect and may compromise the blood supply of the distal flap (Fig. 23-8). Preoperative flap design must account for pivotal restraint to avoid excessive tension, especially if secondary motion would displace a free margin.
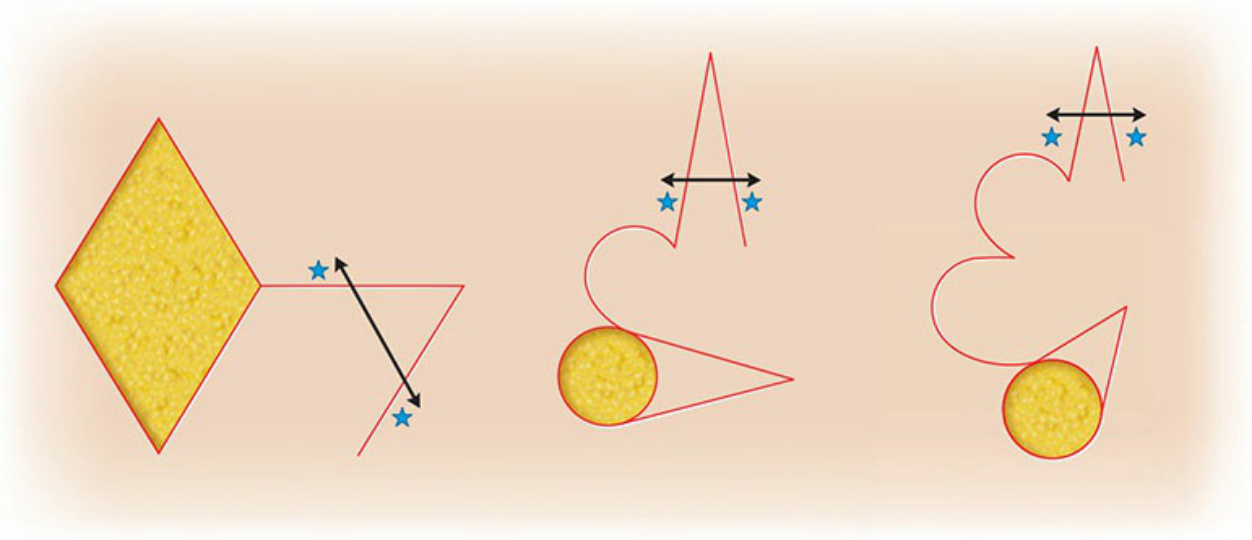
Figure 23-4. Transposition flaps displace tension from the primary defect to the final donor site (stars denote key stitch and arrows demonstrate direction of tension vector).
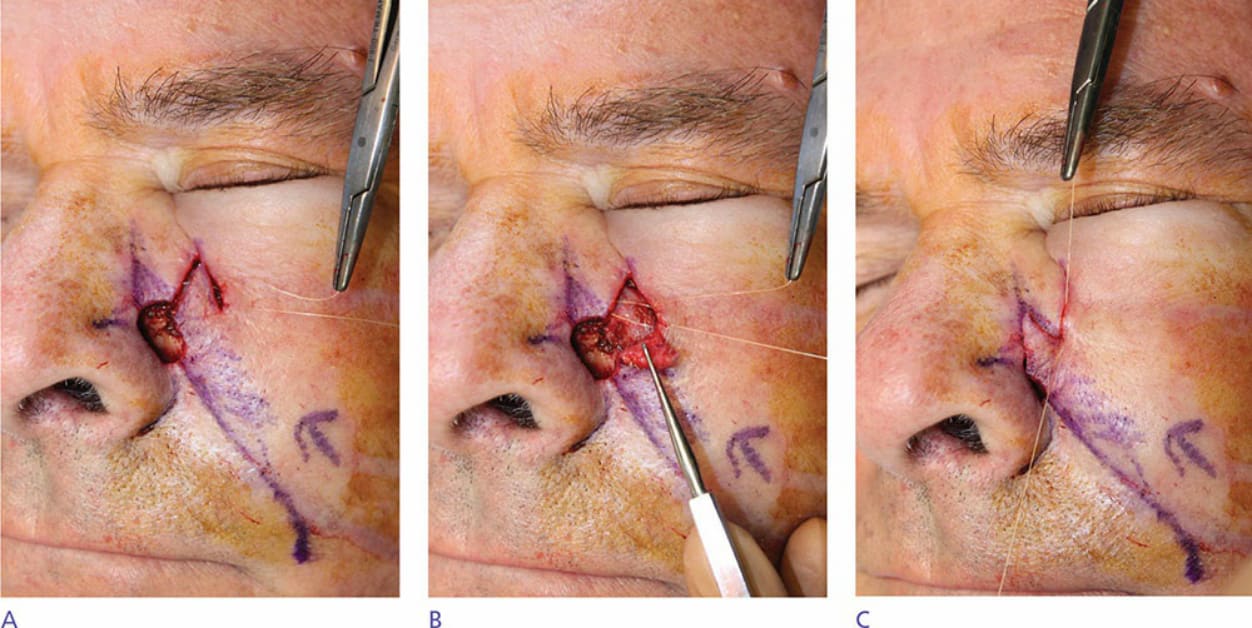
Figure 23-5. Closing the terminal donor site allows transposition of the flap into the primary defect with minimal tension. (A) Rhombic flap designed and incised. (B) The first key stitch closes the donor site. (C) After closure of the donor site, the flap drapes over the primary defect.

Figure 23-6. Secondary motion from suture placement near the inferior lateral orbital rim, where a secondary key stitch would be placed, may risk ectropion. This is mitigated by use of tacking sutures from the undersurface of the flap to the origin of the zygomaticus major, thereby suspending the flap in place and minimizing secondary motion near the vulnerable eyelid.
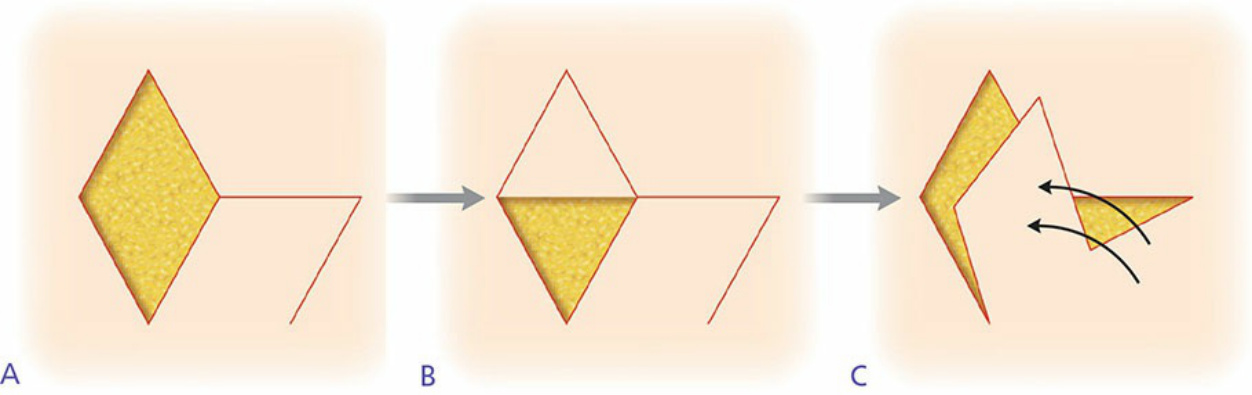
Figure 23-7. A rhombic flap depicted as a rotation flap with a large back cut. As with a rotation flap, a rhombic flap is subject to pivotal restraint both at the base of the defect and at the terminus of the back cut.
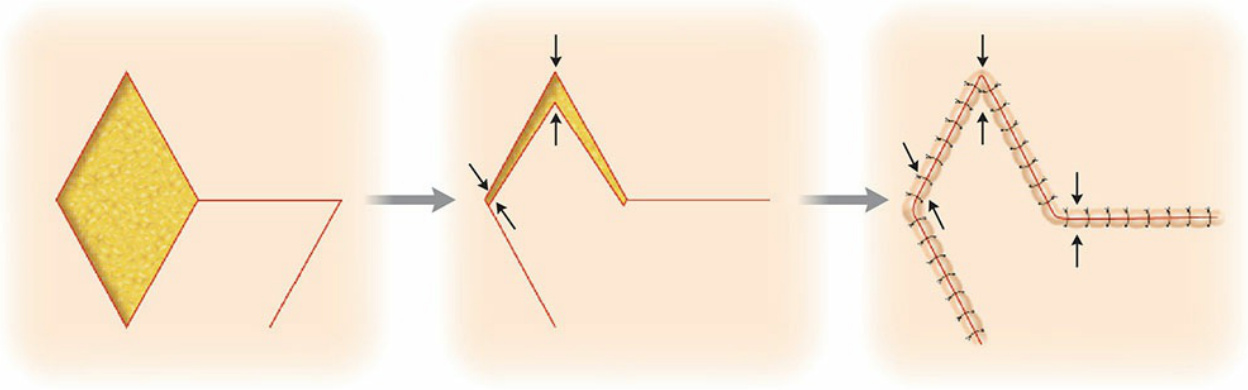
Figure 23-8. If the flap design does not take into account the consequences of pivotal restraint and the recipient site is unable to provide secondary motion, excess tension may compromise blood supply to the distal edges of the flap.