CHEEK
CHEEK
Given the excellent tissue mobility on the cheek, most small- and medium-sized wounds are readily repaired in a primary fashion. However, larger surgical defects or those located near anatomic free margins may benefit from repair with rotation flaps. Large wounds of the preauricular cheek or inferior temple can be nicely closed with broad, medially based rotation flaps utilizing tissue laxity from the lower cheek and neck (Figs. 22-14 through 22-16). These flaps are undermined at the level of the superficial subcutaneous fat. The use of a backcut can aid in the rotation of these flaps or a standing cone deformity can be removed posteriorly around the earlobe to add a component of advancement to their movement. One advantage of this design is that it conceals many of the incision lines along the hairline and within skin folds of the preauricular cheek.
Defects on the superior cheek that are more medially located can be repaired with similarly designed inferolaterally based rotation flaps. Also undermined in the superficial subcutaneous fat, these flaps are rotated superiorly with the long arc of rotation oriented along the nasofacial sulcus. A flaw inherent in this design is the propensity to pull inferiorly on the lower eyelid and create a potential for ectropion. A recent small case series demonstrated that superomedial anchoring of such flaps to the periosteum of the nasal bone or medial maxilla resulted in no occurrences of ectropion.25
The comet flap or dog-ear rotation flap, though useful in a variety of locations on the head and neck, is particularly useful on the cheek. This repair combines a primary closure of one end of the defect with the creation of a rotation flap from the tissue redundancy at the other end of the defect. After it is determined which end of the wound would be optimally closed in a primary fashion, the standing cone deformity is excised
and an intermediate-layered closure is performed to a point at which further closure is not permitted due to excessive tension. The rotation flap is then designed to maximally utilize the tissue redundancy of the standing cone at the opposite end of the wound. The length of the arcuate incision of the flap should be approximately equal to the length of the remaining wound edge to provide for adequate rotation with minimal tension across the secondary defect.26
LIP
Medium-sized defects of the upper cutaneous lip can be nicely reconstructed with a rotation flap elevated just medially to the nasolabial fold (Figs. 22-17 through 22-19). The long arc of rotation is incised along this cosmetic boundary separating the upper lip from the cheek, and the flap is then undermined above the orbicularis oris muscle. The incision line may be extended as far inferiorly as necessary to achieve adequate rotation without distortion of the commissure and vermillion. If required, a standing cone deformity angled medially can be removed around the commissure onto the lower cutaneous lip to prevent unwanted tissue movement. When rotated into position, a standing cone deformity must be removed inferior to defect. If the defect approaches or involves the apical triangle, the flap should be designed and rotated in such a fashion as to recreate this important cosmetic subunit. Fullness of the upper lip and increased show of the vermillion are common in the immediate postoperative period, but this resolves within a week or two in an overwhelming majority of cases. A recent case report demonstrated excellent cosmetic outcomes for defects of 1 to 2 cm in diameter on the lateral upper cutaneous lip.27
A similar flap that recruits tissue from the medial cheek has been effective in closing large defects of the cutaneous upper lip. This technique involves creating a template of the entire upper cutaneous lip subunit, to include the apical triangle, from the unaffected side and transferring it to the medial cheek of the affected side. The flap is then incised, maintaining an inferiorly base pedicle and undermined superficial to the orbicularis oris muscle. Once rotated into place, the flap recreates the entire upper cutaneous lip lateral to the philtral column. The lateral border of the flap recreates the nasolabial fold. Finally, the secondary defect on the cheek is repaired primarily.28

Figure 22-14. Rotation flap repair of a lateral cheek defect. Given the size of the defect, tissue recruitment from the ipsilateral jowl and submental skin is required. The defect size was narrowed first with a superior standing cone.
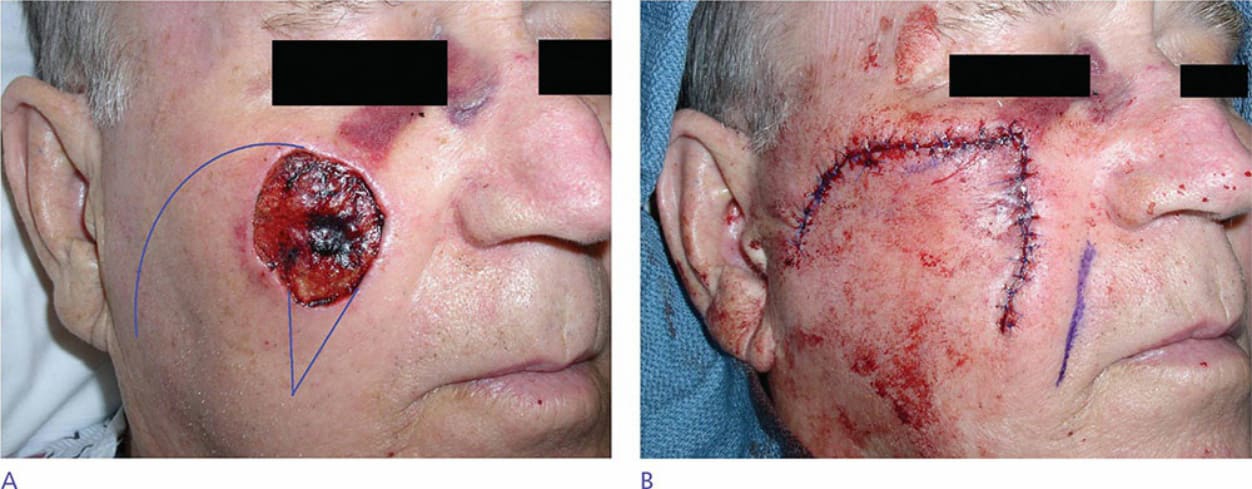
Figure 22-15. Large defect of the central cheek closed with a laterally based rotation flap. Note that the standing cone is oriented parallel to the nasolabial fold for optimal cosmesis.

Figure 22-16. Very large centromedial cheek defect. A large, laterally based rotation flap is designed to recruit from the lateral cheek, jowl, and submental skin. Once again, the inferior standing cone is placed within the nasolabial fold to preserve the cosmetic subunit.

Figure 22-17. Defect of the right upper cutaneous lip–nasolabial fold repaired with a rotation flap. (A) Preoperative appearance. (B) Postoperative appearance.

Figure 22-18. Rotation flap of the lateral upper cutaneous lip (“Hatchet flap”). Note the rotation flap is designed such that the rotational arm of the flap recreates the nasolabial folds and the standing cone lines within the vertical perioral furrows.

Figure 22-19. Left upper lip rotation flap involving the vermilion border. (A) Preoperative appearance. (B) Postoperative appearance.