EYELID AND INFRAORBITAL REGION
EYELID AND INFRAORBITAL REGION
Large rotation flaps recruiting tissue laxity from the temple and cheek have been used to close surgical defects of the lower eyelid for nearly a half century. In 1966, Mustarde initially described a large rotation flap where a long, sweeping incision is made laterally along the lower eyelid–cheek junction, coursing superolaterally onto the temple and then inferiorly along the preauricular cheek.16 Coined the “Mustarde flap,” this reconstructive option has proved to be useful for large defects of the medial cheek and lower eyelid (Fig. 22-12). In 1970, Tenzel described a semicircular rotation flap from the temple of similar design and movement. This flap also incorporated the
orbicularis oculi muscle and was intended for repair of full-thickness defects of the central or lateral lower eyelid.17 The movement of the Tenzel flap is further aided by a lateral canthotomy and cantholysis. Wounds up to two-thirds of the width of the lower eyelid can be repaired with this method.
As with many other rotation flaps, both of these flaps utilize advancement in addition to the primary motion of rotation. The tension vector along the leading free edge of the flap is oriented medially, while tension on the trailing edge is directed superiorly and laterally toward the temple and preauricular cheek. Very little tension in directed inferiorly, minimizing undesired distortion of the free margin of the lower eyelid. As
stated previously, the length of the arc of any rotation flap is inversely proportional to the tension across the secondary defect. The long incision lines of these flaps further ensure minimal tension across the secondary defect and mitigate the potential for ectropion. However, Mustarde himself recognized that large rotation flaps from the cheek have a tendency to sag over time given the added tissue bulk carried forward onto the lower eyelid.18 He advocated for the use of both deep tacking sutures and septal cartilage grafts to support the lower eyelid.
Numerous modifications to these basic designs have been described. The use of a Zplasty at the lateral aspect of these flaps has been advocated as a means to push them medially. This effectively serves to resist the natural tendency of the tissue to recoil laterally. Additionally, inverted forms of the semicircular flap have been shown to be useful in repairing similar defects of the upper eyelid.19 Rao and Frank described a modification of the Mustarde flap which is helpful for repair of medial eyelid defects. It incorporates the standing cone typically created inferior to the defect as a Burow’s graft to repair the noneyelash-bearing margin medial to the lower lacrimal punctum.20 Purely cutaneous defects of the lower eyelid are very amenable to repair with a modification of Tenzel’s semicircular flap. The principle design and tissue movement are identical to the original flap and they still require a superior arcuate extension to avoid unwanted secondary motion of the eyelid inferiorly. However, this flap modification is cutaneous only, being elevated above the level of orbicularis oculi, whereas the flap was musculocutaneous in its initial description.
Large temple and cheek rotation flaps are not without shortcomings. As mentioned, the primary concern with these flaps is support of the lower eyelid and prevention of downward tension that may result in ectropion. Both oversizing of the flap with broad superolateral arcuate incisions and the use of suspension sutures helps combat this potential pitfall. The Mustarde flap particularly relies on laxity from the preauricular cheek. If this laxity is not present, unwanted tension may occur with rotation and predispose to distal flap necrosis.19 Additionally, long-lasting eyelid edema is common owing to the disruption of the local lymphatic system. Finally, textural mismatch of the thick skin of the cheek and the thinner skin of the eyelid can also present challenges. This may be compensated for with appropriate thinning of the flap edge and careful suturing technique.
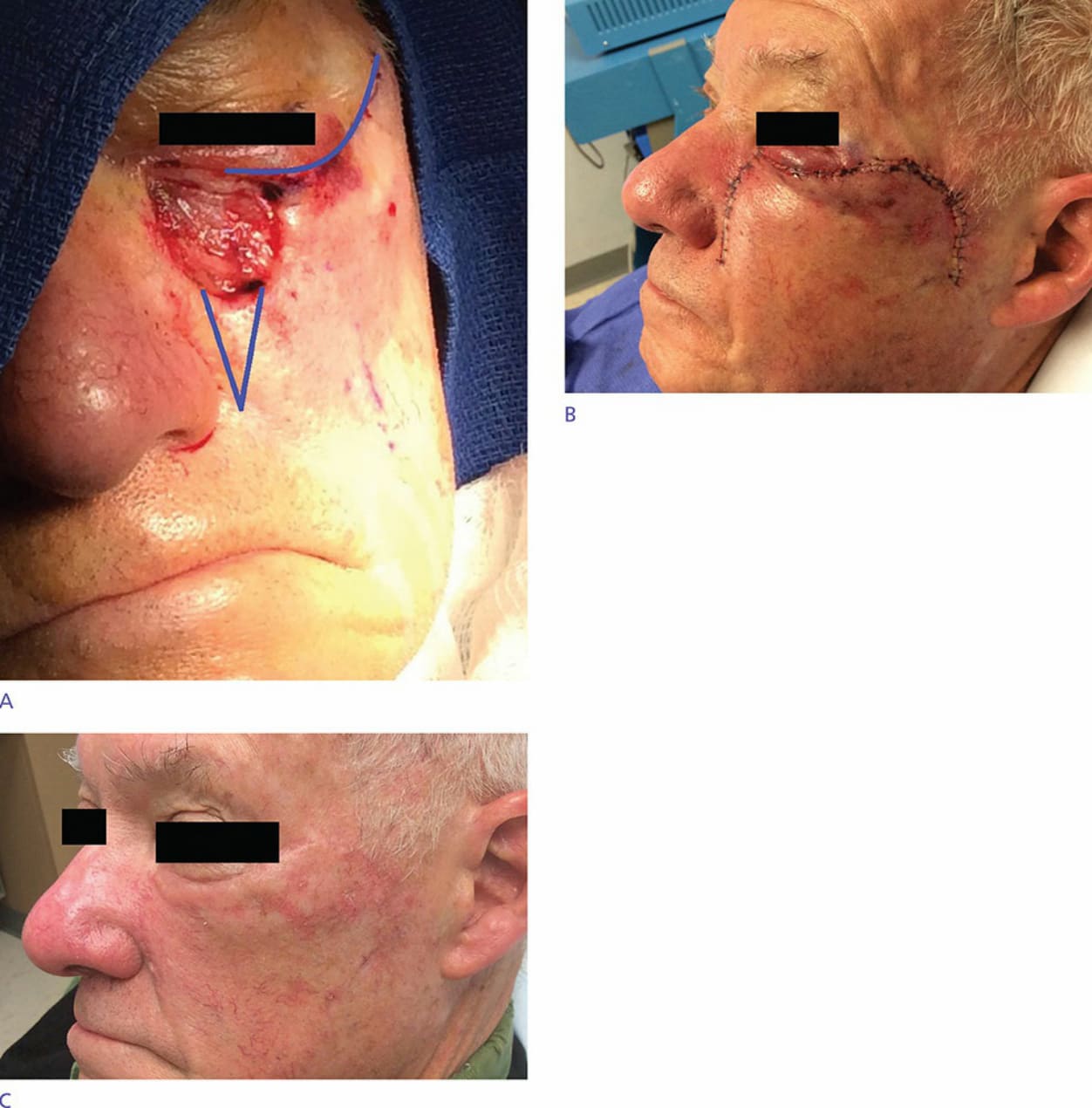
Figure 22-12. Classic cheek rotation “Mustarde” flap—this classically described rotation flap is useful in the repair of large medial lower eyelid and upper medial cheek defects. A long, sweeping incision along the inferior eyelid, and extensive undermining is performed. Immediate postoperative and long-term postoperative results are shown as well with excellent cosmetic results. Redundancy along the nasofacial groove usually requires removal as a standing cone. Postoperatively, eyelid edema and lack of sensation are common findings.