Other nasal rotation flaps
Other nasal rotation flaps
A variety of other rotation flaps add to the cache of repairs for nasal reconstruction. A traditional rotation flap can be very useful in small- to medium-sized defects on the distal nasal sidewall, particularly those located just superior to the alar crease (Figs. 22-7 and 22-8). For such defects, a laterally based rotation flap utilizes tissue laxity from the sidewall superolateral to the wound, while also orienting the resultant standing cone along the alar crease. Similarly, traditional rotation flaps can be used to repair small defects of the middle-third of the ala located just below the alar crease. From the defect, incising laterally and inferiorly along the alar crease creates a rotation flap that is confined to the alar subunit. Once rotated medially, it provides excellent tissue coverage and match without adversely affecting the free margin of the alar rim.
Similar to a traditional rotation flap from the nasal sidewall, Hafiji et al. described a laterally based rotation flap from the nasal sidewall as an alternative to a bilobed flap for the repair of lateral nasal tip defects. Coined the “advancement and inferior rotation of the nasal sidewall (AIRNS)” flap, it incorporates advancement from the medial canthal region and rotation from the nasal sidewall to repair defects of just over 1 cm. It also has the benefit of directing the standing cone deformity nicely along the alar crease.9
The spiral flap is another rotation flap elevated from the nasal sidewall that, in addition to simple rotation, can be utilized to repair defects involving or just below the alar crease (Fig. 22-9). This flap utilizes the relatively narrow flap tip folded back upon itself allowing preservation of the alar crease. As described by Mahlberg et al., this flap is useful for reconstructing defects of the alar groove and alar body of 5 to 15 mm in diameter.10 Not only does this flap offer the benefits of a single-stage repair with excellent local tissue color and texture match, it also reliably recreates the alar groove. Careful attention must be paid to preserving a broad pedicle, as there is a tendency when designing this flap to increase the length-to-width ratio which may predispose it to distal tip necrosis. This can be done by designing the flap as a logarithmic spiral as opposed to a classic Archimedean spiral.
A novel medially based rotation flap was reported by Bryan et al. for small- to medium-sized defects of the middle-third of the alar crease. Dubbed the “wave” flap, it shares elements of both a medially based hemi-nasal rotation flap and the spiral flap. Like a medially based hemi-nasal flap, it touts a broad pedicle and practicality for lateral nasal defects. Yet, similar to the spiral flap, the distal tip is turned back onto itself and cosmetically recreates the alar crease. One benefit of this flap over the spiral flap is that the majority of its incision lines are camouflaged within the nasofacial sulcus.11
Similar to the spiral and “wave” flaps, the “shark” island pedicle flap also takes advantage of rotating a portion of the flap back on itself to help recreate the alar crease (Fig. 22-10). It is particularly useful in reconstructing combined alar and medial cheek defects. This flap can be thought of as having two distinct components. The trailing portion of the flap is very similar to a traditional V-to-Y island pedicle flap. It is a random pattern flap of a long triangular shape oriented along the nasolabial fold that derives its blood supply from perforators of the angular artery. To this traditional island pedicle flap, the shark flap adds a leading portion that extends around the defect both superiorly and proximally. This small isthmus is a myocutaneous flap incorporating fibers of the levator labii superioris and should be designed to be the same width as the alar portion of the defect. As the trailing portion of the flap is advanced and the secondary defect is closed behind it, the leading portion is rotated between 90 and 180 degrees back on itself. This creates an inverted standing cone and suture line that create the alar crease.12
The Peng flap, later modified by Rowe, is both a bilateral rotation flap and a direct advancement flap that recruits tissue from both nasal sidewalls and the glabella, respectively (Fig. 22-11). It is useful for nasal tip defects or defects straddling the cosmetic subunit boundary between the nasal tip and distal nasal dorsum of up to approximately 2 cm.13,14 Incisions are made from the medial canthus inferiorly along the nasofacial sulcus to the distal aspect of the defect. The bilateral flap is then undermined and elevated deep to the nasalis muscle and then rotated medially to meet each other. A standing cone deformity is removed superiorly along the nasal dorsum. A more recent modification advocates for incising the distal portion of the flaps along the alar crease to better hide suture lines within subunit boundaries. Additionally, the cheeks can be advanced bilaterally to assist in the closure of the secondary defect with the removal of crescentic standing cone deformities along the alar crease as needed.15

Figure 22-7. Rotation flap repair of the supra-alar nasal sidewall with good cosmetic outcome. Although not represented in this repair, it is paramount to consider distortion of the ipsilateral alar rim when designing an adjacent rotation flap.

Figure 22-8. Medially based rotation flap for a lateral nasal sidewall defect. The glabella provides an ample tissue reservoir in this scenario within limited potential for webbing of the medial canthus.
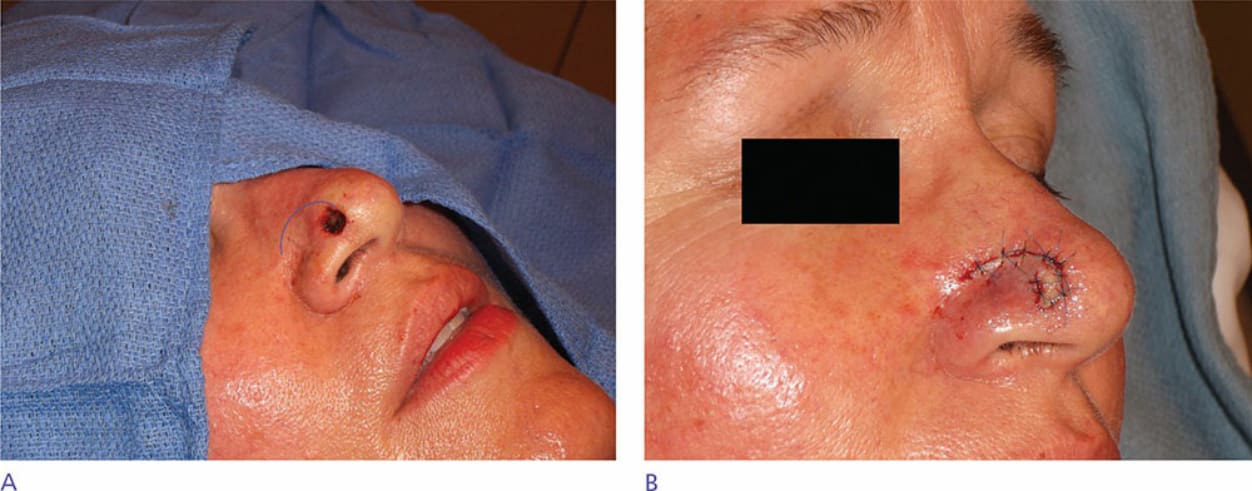
Figure 22-9. Spiral flap—the spiral flap is a useful repair option for small defects of the superior ala. The leading tip of the flap is folded upon itself, allowing for accurate recreation of the alar groove. Caution must be taken to avoid undue tension on the tip as it is particularly susceptible to necrosis and strangulation.
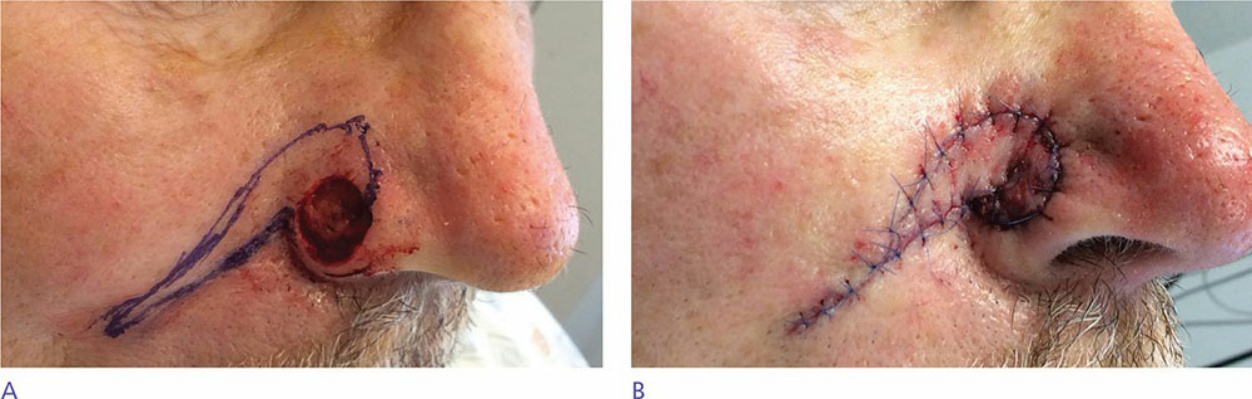
Figure 22-10. Shark-island flap—a variant on the spiral flap which recruits from the medial cheek and nasolabial fold. Again, tip necrosis is a concern, and measures to avoid excess tip tension are paramount to success.
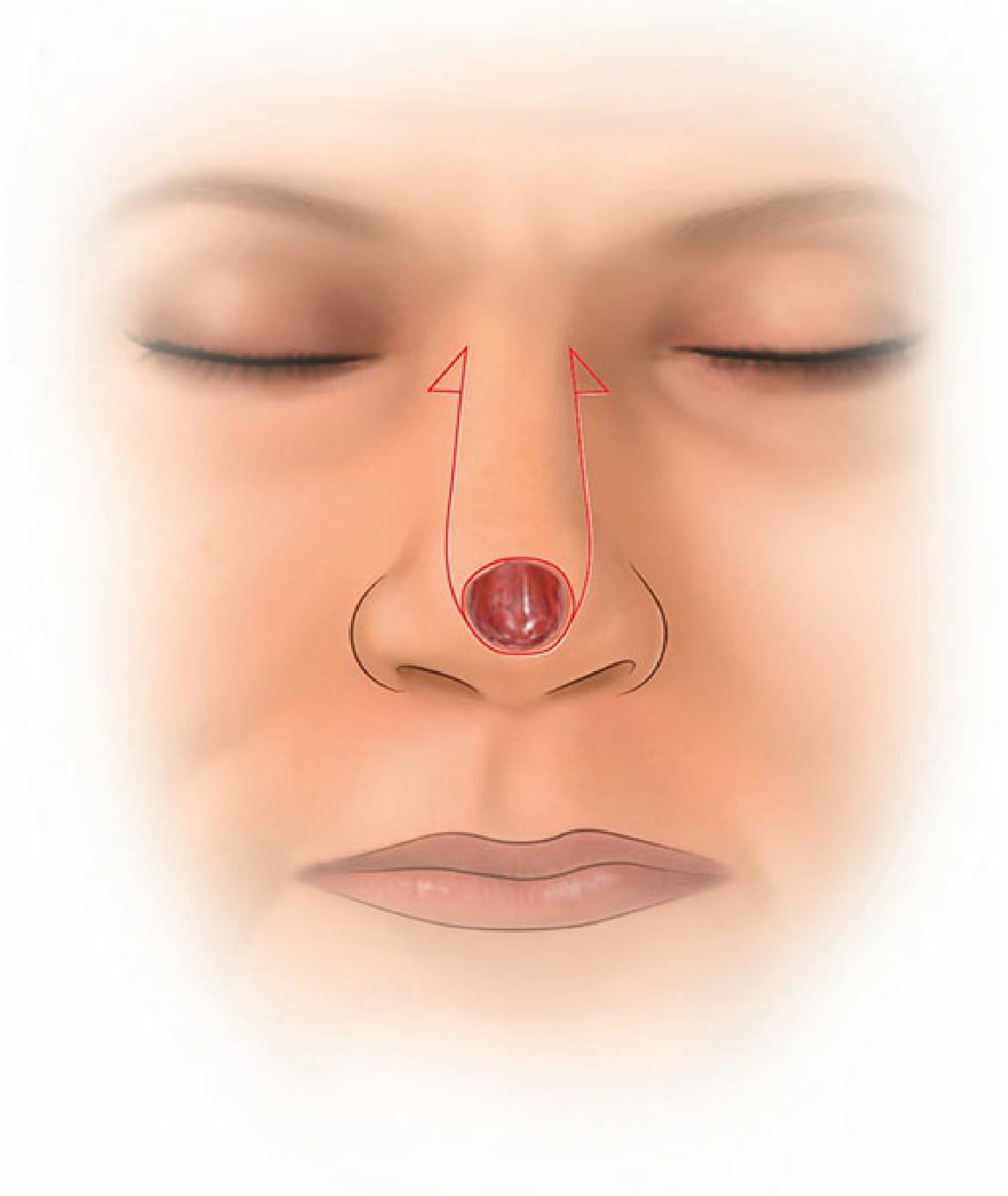
Figure 22-11. The Peng flap.