Dorsal nasal rotation flap
Dorsal nasal rotation flap
In 1967, Rieger described the dorsal nasal rotation flap as a means for closing mediumto large-sized defects on the distal nose measuring up to 2 cm in diameter (Fig. 22-4).4 This flap utilizes tissue laxity on the upper nose and glabella. Marchac and Toth modified this flap by removing a standing cone vertically oriented from the superior aspect of the defect into the flap pedicle.5,6 Due to the rich blood supply of the flap, the authors argued that the flap was amenable to a shortened flap base in favor of greater
mobility. Rigg described a variant of the dorsal nasal flap termed the heminasal flap that is particularly useful for smaller defects of the distal nose.7 The heminasal flap has the benefit of utilizing only a portion of the nasal skin. Depending on the location of the defect, the location of the free edge of the flap and the pedicle can be adjusted. For example, the free edge of the flap would be oriented along the nasal midline for more medial defects, whereas lateral defects would be more readily repaired with the free edge directed along the nasofacial sulcus.
This flap and its modified versions are executed in a very similar fashion (Figs. 22-5 and 22-6). Initially, a broad sweeping incision is made from the glabella and carried downward past the medial canthus and along the nasofacial sulcus to the distal aspect of the defect. For purely midline defects, the pedicle may be based on either side of the nose. For defects that are even slightly lateral of midline, a contralateral pedicle is desired. A backcut of 30 to 45 degrees is made in the glabella to further aid in rotation. A general strategy for determining the height of the glabellar component of the flap is to measure 1.5 to 2 times the height of the nasal tip defect.8 The nasal component of the flap is then elevated just above the level of the periosteum and perichondrium. Undermining of the flap continues across the nasal dorsum to the contralateral nasofacial sulcus. When undermining the flap in the glabella, the level is superficial to procerus and corrugator supercilii muscles to prevent unnecessary disruption of motor function in this region. Once adequate hemostasis is obtained, the flap is rotated into place. The secondary defect in the glabella is typically closed first in a layered fashion. As the flap is rotated, the glabellar portion of the flap usually becomes redundant and is trimmed. Careful planning and sizing of the flap as well as undermining of the
surrounding tissue are necessary to prevent asymmetry. Oversizing of the flap is often utilized to prevent undesired distortion of the nasal tip. Additionally, a longer, broader arc of rotation can prevent pull on the contralateral medial canthus and ala.
There are several advantages of the dorsal nasal rotation flap. First, it provides good local tissue match for both color and texture. This flap also generally respects cosmetic subunit boundaries. Most of the suture lines fall within the glabellar furrows, the nasofacial sulcus, and the alar creases. Additionally, the robust blood supply derived from angular artery perforators contributes to excellent flap viability. Finally, this flap
has the benefit of being a single-staged repair.7 The primary disadvantage of this flap is its large size, as much of the skin of the nose must be elevated to achieve adequate tissue movement and coverage.
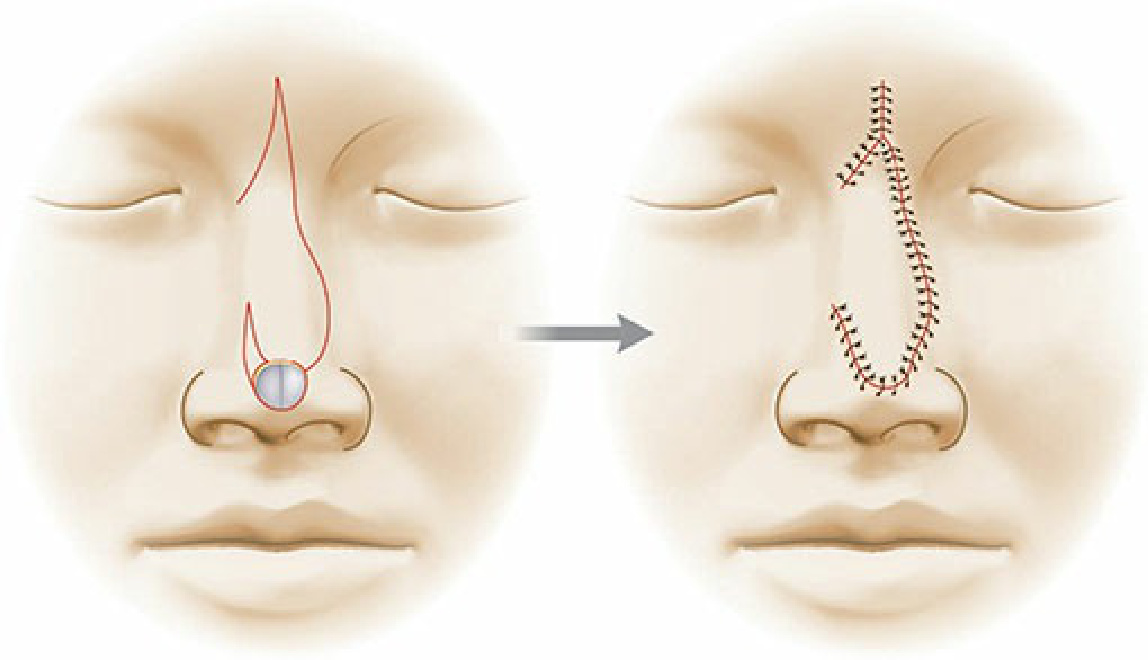
Figure 22-4. The dorsal nasal rotation flap. Note the use of a large backcut in the glabellar area to better mobilize the flap.
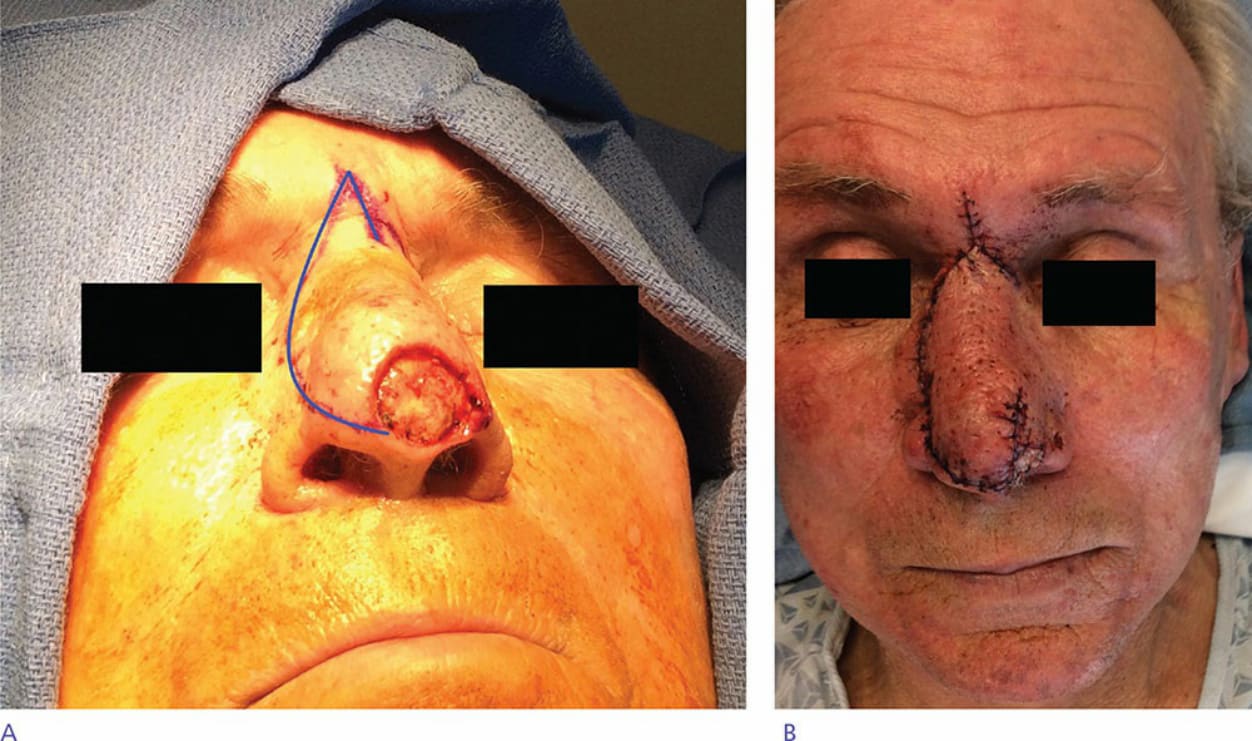
Figure 22-5. Dorsal nasal rotation flap (“Reiger flap”)—defect of right nasal tip and supratip greater than 1 cm. A sweeping incision designed along the nasal sidewall and extending to the glabella with a backcut. The flap is rotated inferomedially, and the trailing edge of the flap is closed in a V-Y fashion.

Figure 22-6. Heminasal variant of dorsal nasal rotation flap—this flap was limited to one-half of the nasal dorsum and sidewall, achieving significant tissue recruitment from the ipsilateral nose and glabella.