FLAP DYNAMICS AND DESIGN
FLAP DYNAMICS AND DESIGN
As with the design of any flap, it must first be determined which tissue reservoir will be recruited. A rotation flap is, by definition, a sliding flap. The tissue reservoir must be immediately adjacent to the defined surgical defect. When choosing a tissue reservoir, cosmetic subunits and potential distortion of free margins must be taken into
consideration. Once the most appropriate reservoir has been identified, a curvilinear arc is extended from the wound around a central pivot point. Ideally, this arcuate incision may lie within a relaxed skin tension line, though this is not always possible. After the flap is incised, the flap, primary, and secondary defects are all widely undermined. The flap can then be rotated inward to fill the primary defect (Fig. 22-1).
At this point, there are two areas where tissue redundancy becomes evident—the pivot point adjacent to the primary defect and the flap base at the end of the arcuate incision. Pivot point redundancy can be removed as a standing cone either before (“triangulating” the defect) or after the inset of the flap, and flap base redundancy oftentimes can be redistributed by meticulous “rule-of-halves” suturing or removed as a standing cone. This redundancy may or may not be significant, depending on the site and size of the defect.
A critical consideration in flap design is sizing of the flap. All rotation flaps are subject to rotational shortening and pivotal restraint—as the flap tip rotates inward to fill the primary defect, the arc length of the flap decreases. This is due to tissue restraint at the flap base. In clinical practice, two basic designs create the initial construct for most rotation flaps. These designs primarily differ in arc length of the flap tip and takeoff point. The arc of rotation for a standard rotation flap classically begins tangentially to the defect. With the forces of pivotal restraint, the flap tip is shortened
upon rotation into the defect, and the tip must be advanced upward to completely fill the gap. As a result, a degree of tension is transferred to the flap tip, already the area most susceptible to necrosis. To combat this design flaw, Dzubow described a vertical offset or a “step-up” of the takeoff point of the flap.1 In other words, this modification extends the length of the leading edge of the flap past the surgical defect, and can be thought of as “oversizing” the flap (Fig. 22-2). This approach allows the rotation flap to fill the defect under minimal tension on the flap tip. However, increasing the length of the leading edge of the flap will result in a larger secondary defect, which may be undesirable depending on the cosmetic subunit. This, in turn, will increase the tension across the secondary defect and must be accounted for. This exchange of tension between the two designs was nicely demonstrated by Lichon et al. in vivo using pig models and tension-measuring devices.2
Additional modifications to rotation flap features can aid in tissue movement and redirect tension vectors. The use of a backcut can further reduce pivotal restraint and assist in rotating the flap into place (Fig. 22-3). However, careful attention must be paid to the length of a backcut that is utilized. A backcut inherently reduces the width of the
pedicle and may compromise flap perfusion. The overall length of the arc of the rotation flap is also a key component. Specifically, the arc length of rotation is inversely proportional to the closure tension across the secondary defect. This concept must not be overlooked when free margins are in close approximation of the planned secondary defect. Finally, the total angle of rotation should be considered. In vivo studies have shown that generally 90 to 135 degrees of rotation is appropriate. More obtuse angles of rotation do not improve, and may in fact hinder, tissue movement.3
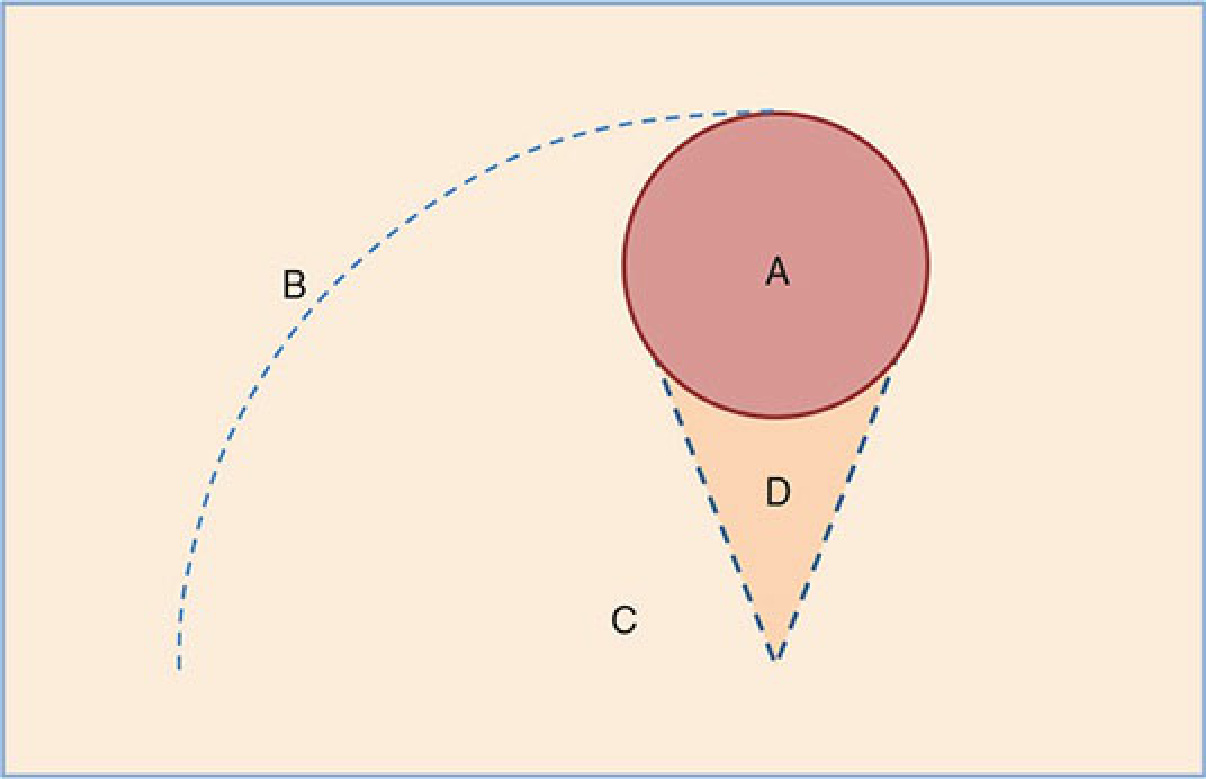
Figure 22-1. Rotation flap geometry. (A) The primary surgical defect is denoted by the red circle. After determination of the tissue recruitment area, a sweeping curvilinear arc is carried away from the primary defect with a tangential start point (B) around a central pivot point (C). Tissue redundancy can be anticipated adjacent to the pivot (D), and oftentimes is removed preemptively as a standing cone.
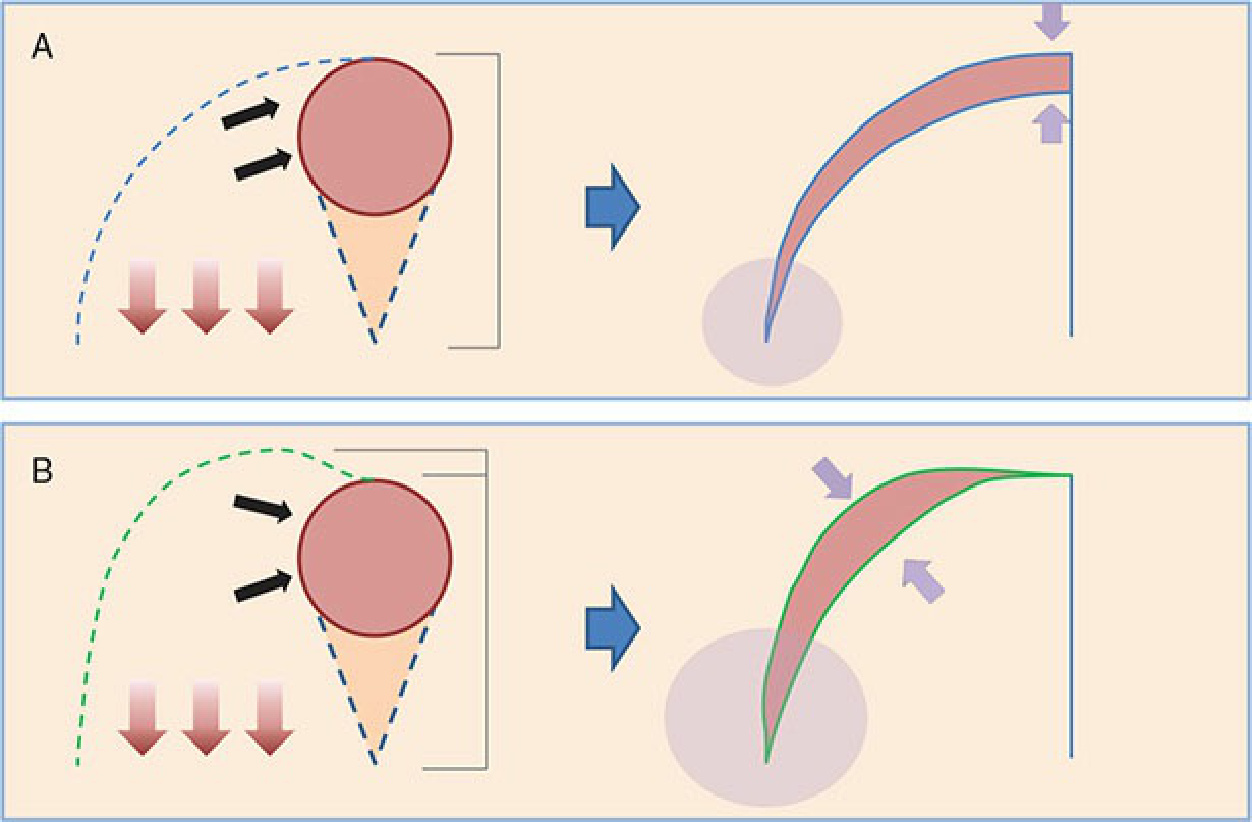
Figure 22-2. Rotational shortening. (A) Rotation flap designed with “traditional” tangential takeoff angle. Pivotal restraint effectively shortens the flap tip as it moves through the arc of rotation, and places additional tension on the tip once the flap movement is complete. (B) Oversized rotation flap design overcomes rotational shortening but creates a larger secondary defect and potentially creates more tissue redundancy. Black arrows, primary flap movement; red arrows, vector of pivotal restraint; purple arrows, the greatest area of tension on secondary defect; purple circles, potential tissue redundancy.
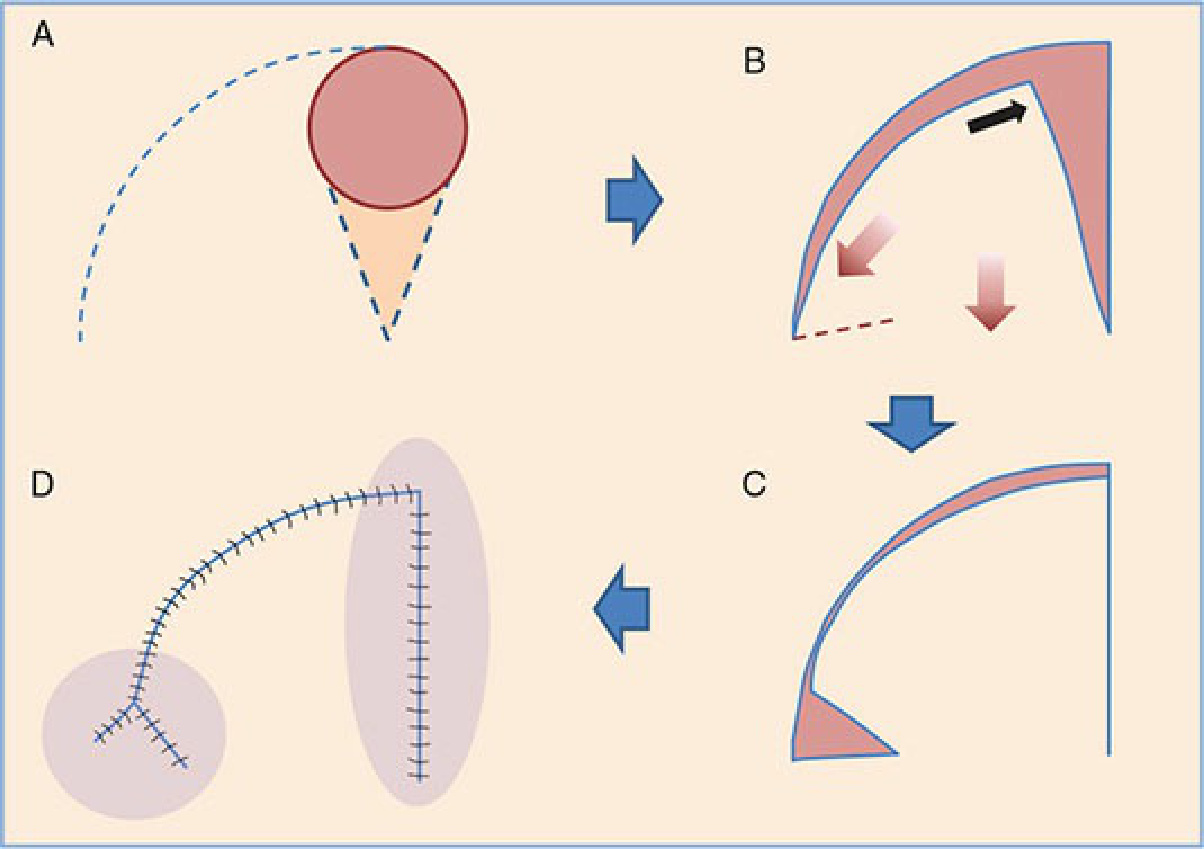
Figure 22-3. Backcut modification. (A) A standard rotation flap is designed, but occasionally excess laxity is needed to complete the rotation. (B) A backcut is designed and incised. (C) This allows the completion of the rotation arc. (D) Final closure—the secondary defect of the backcut is closed in a V-Y fashion. Black arrow, primary flap movement; red arrows, tissue restraint vectors; purple circles, tension on final closure.