Displacement of free margins
Displacement of free margins
Whenever an advancement flap is adjacent to a free margin, the surgeon must be careful to keep from “pulling” or “pushing” the margin out of position. To avoid “pulling” on a free margin, the primary tension vector for closure should be parallel to the free margin. “Pushing” may occur when the opposing sides of the advancement flap that come into apposition are significantly longer than the length of the original tissue that is being resurfaced, similar to the phenomenon that occurs with fusiform linear closures.18
Postoperative complications such as edema, bleeding, or tension can cause ectropion of the lower eyelid. Late ectropion is typically secondary to poorly designed flaps that “pull” on the lower eyelid (e.g., the tension vector for wound closure has a component that is oriented perpendicular to the eyelid margin), scar contraction, or insufficient replacement of the anterior lamella with an undersized graft or flap. Skin grafts and canthal tightening procedures are often used to repair ectropion. Intraoperative assessment of lower eyelid position may help to avoid ectropion. The surgeon can ask patients to open the mouth widely, open the eyes widely, and look up, a position that maximizes stress on the anterior lamella of the lower eyelid (Fig. 21-24). As edema secondary to local anesthesia may temporarily alter free-margin position during surgery, careful preanesthesia planning is of paramount importance.
Advancement flaps from the cheek for defects on the nasal dorsum or sidewall are a reliable option for reconstruction (Fig. 21-25). However, for defects that extend below the peak of the alar groove, advancement flaps from the cheek may result in superior displacement of the nasal tip and alar rim. For these defects, other reconstructive options should be considered to avoid free-margin displacement.
“Bulldozing,” or the appearance of downward displacement of the lateral portion vermillion cutaneous junction (white line), may occur when an advancement flap along the white line does not account for the difference in the vertical position of the medial white line compared to the lateral white line (Fig. 21-26). Especially in patients with a larger slope to their vermillion–cutaneous junction (usually younger patients and women), an ill-planned advancement flap may bulldoze the vermilion inferiorly (Fig. 21-27). Anticipating this eventuality, a small wedge can be removed at the vermilion– cutaneous junction prior to closure, avoiding the need for a secondary revision procedure.
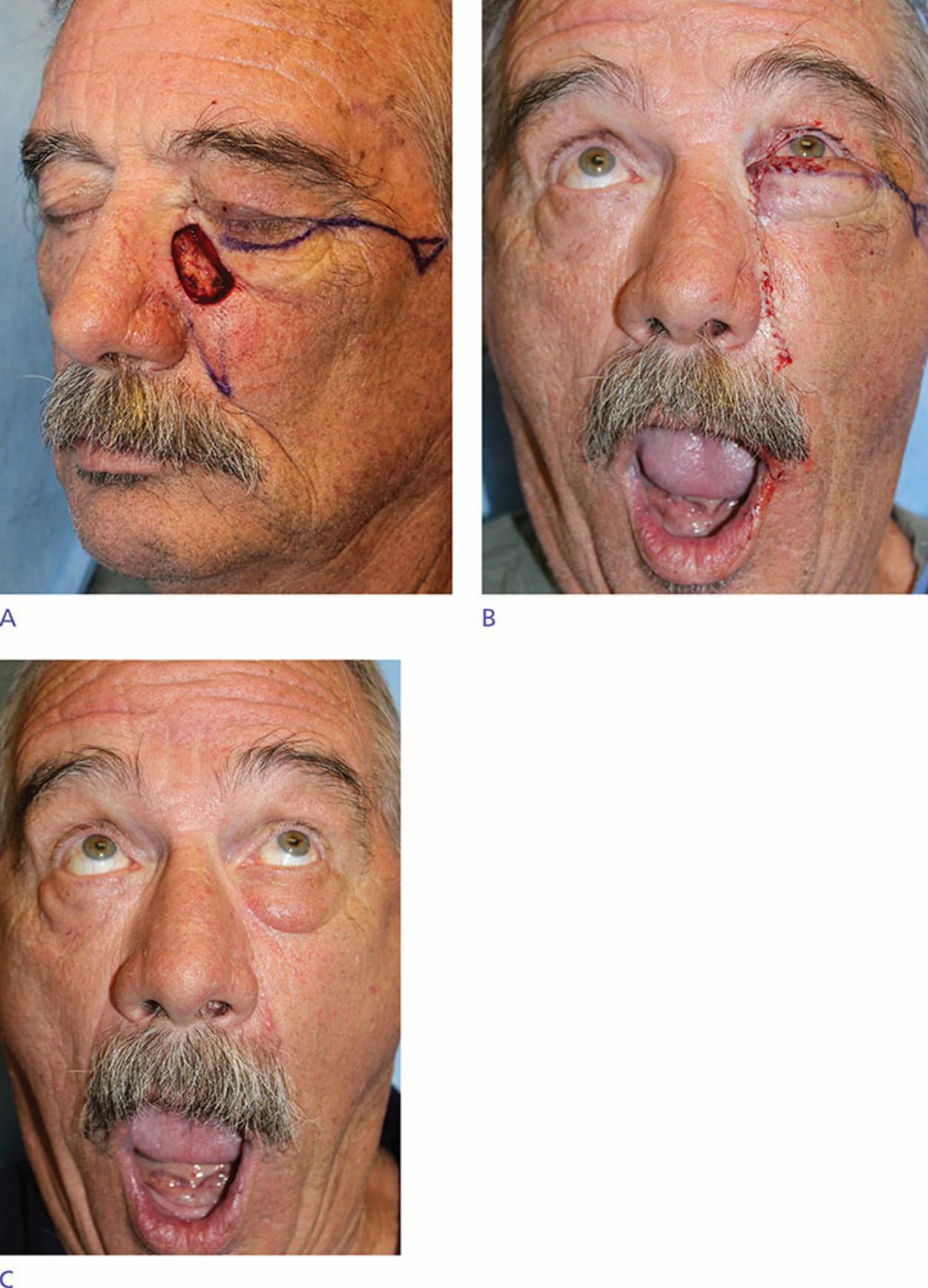
Figure 21-24. Defect after removal of basal cell carcinoma on the medial cheek and lower eyelid after two stages of Mohs surgery (A). The wound was reconstructed with an O-to-L type advancement flap, and no immediate postoperative ectropion was present even with the patient placing stress on the anterior lamella by opening his eyes and mouth (B). At 10 weeks, he continued to have lower eyelid edema (C). This resolved spontaneously over the following 3 months, and he declined further in-office follow-up.

Figure 21-25. Defect with inferior edge above the peak of the alar groove (A). Advancement flap designed (B). Four-month postoperative result with preservation of the position of the alar rim (C).
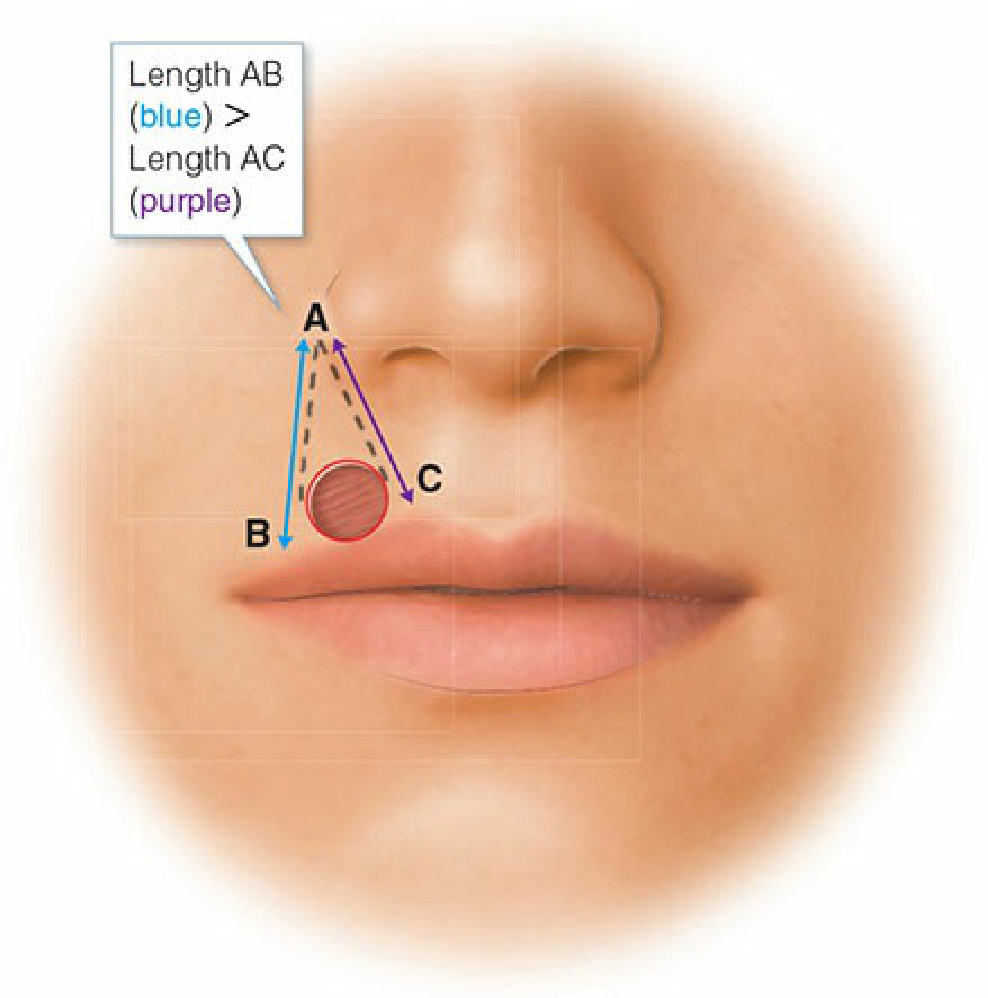
Figure 21-26. The geometry of upper lip bulldozing. The discrepancy between the vertical position of the medial white line compared to the lateral white line may lead to downward displacement of the lip.

Figure 21-27. Defect after removal of a basal cell carcinoma with two stages of Mohs surgery in a 31-year-old female. Note the relatively steep slope of her vermillion–cutaneous junction (A). Immediate postoperative appearance after advancement flap closure (B). Postoperative appearance at 5 months with “bulldozing” or “hooding” of the right lateral vermillion lip by the advanced tissue (C).