Unilateral advancement flap (O-to-U)
Unilateral advancement flap (O-to-U)
This classic unilateral advancement flap is often used for eyebrow defects, eyelid defects, and forehead defects (Fig. 21-15). The principal disadvantage of this advancement flap design is that the advancing edge of the flap may be quite distant from the vascular pedicle, depending on the degree of undermining. However, if the vascular supply is robust, successful results can be achieved even with high length-to-width ratios.
A common variation of this approach is the helical rim advancement flap (Figs. 25- 16 and 25-17). This technique is useful for even fairly large defects on the helix, and the robust blood supply available to this flap has been described.6
The classic unilateral advancement flap may also be used in areas that are not traditionally approached with this technique, such as the cutaneous lip (Fig. 21-18).
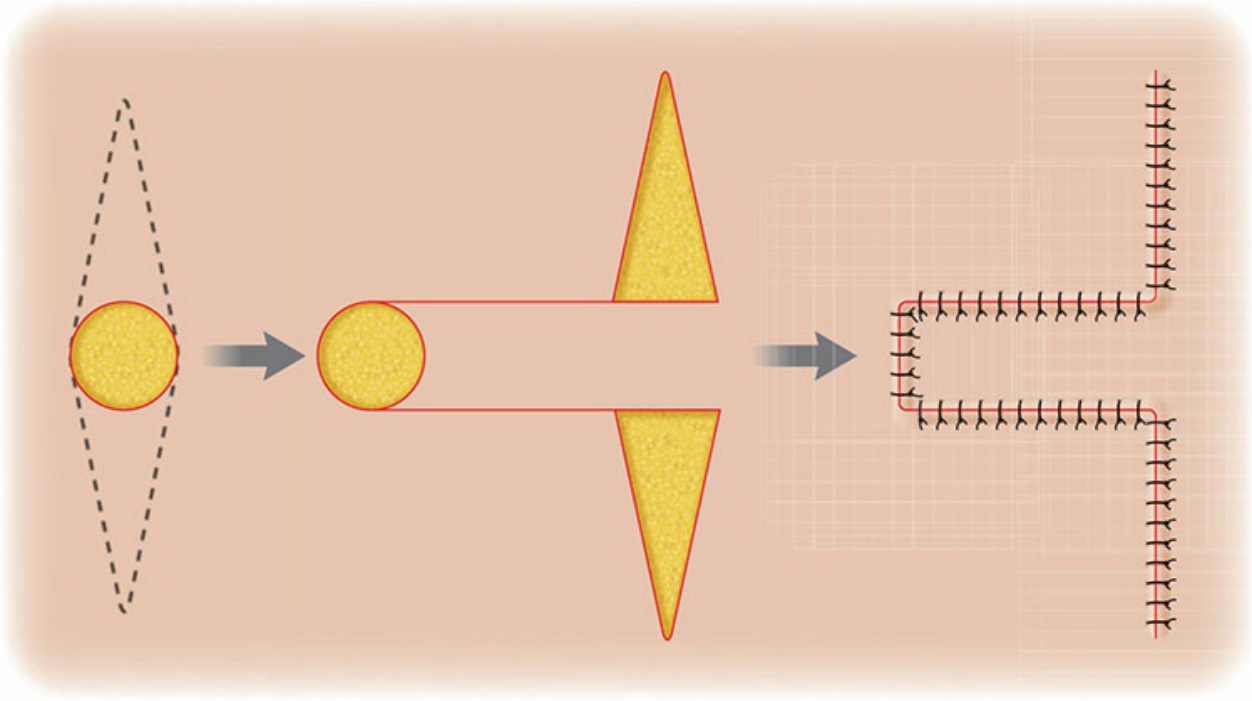
Figure 21-15. O-to-U flap design. Unidirectional primary tissue movement and two standing cones displaced.
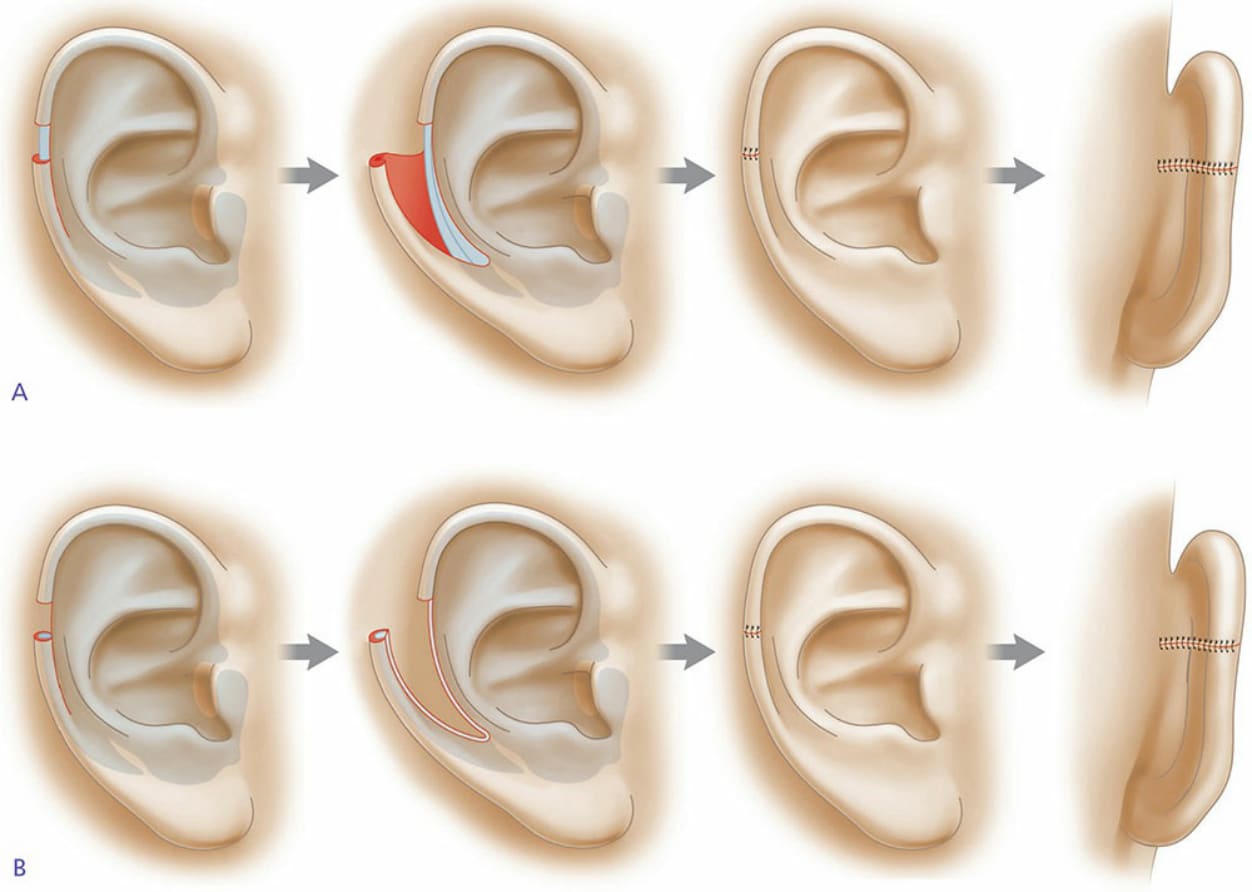
Figure 21-16. Schematic of helical rim advancement. A. A typical helical rim advancement flap. An incision is created along the anterior surface of the ear and carried into the lobule where a medial standing tissue cone is removed. The tissue is reflected off the cartilage and maintained on a posterior pedicle. The flap is advanced and the helical rim is approximated with eversion. A standing tissue cone is removed on the posterior surface of the ear. B. A chondrocutaneous advancement flap. Incision is carried out through cartilage and the flap is advanced and rotated into place. The inclusion of cartilage may be of greater benefit when the defect is higher on the helix or when more cartilage has been lost in the operative wound.
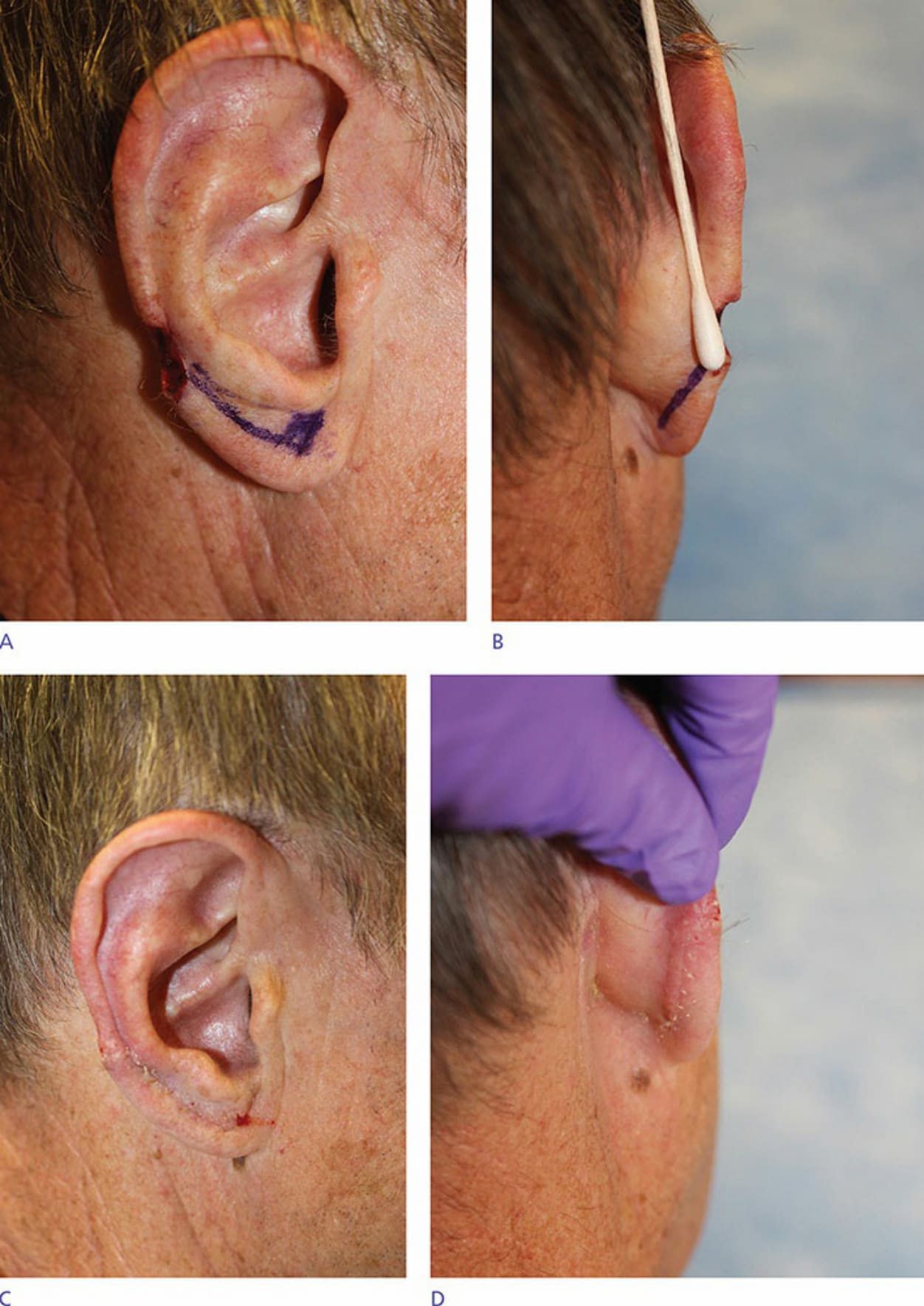
Figure 21-17. Defect and advancement flap design (A,B) with full-thickness incision planned through the helical rim for reconstruction. The 4-week postoperative result is shown (C,D).
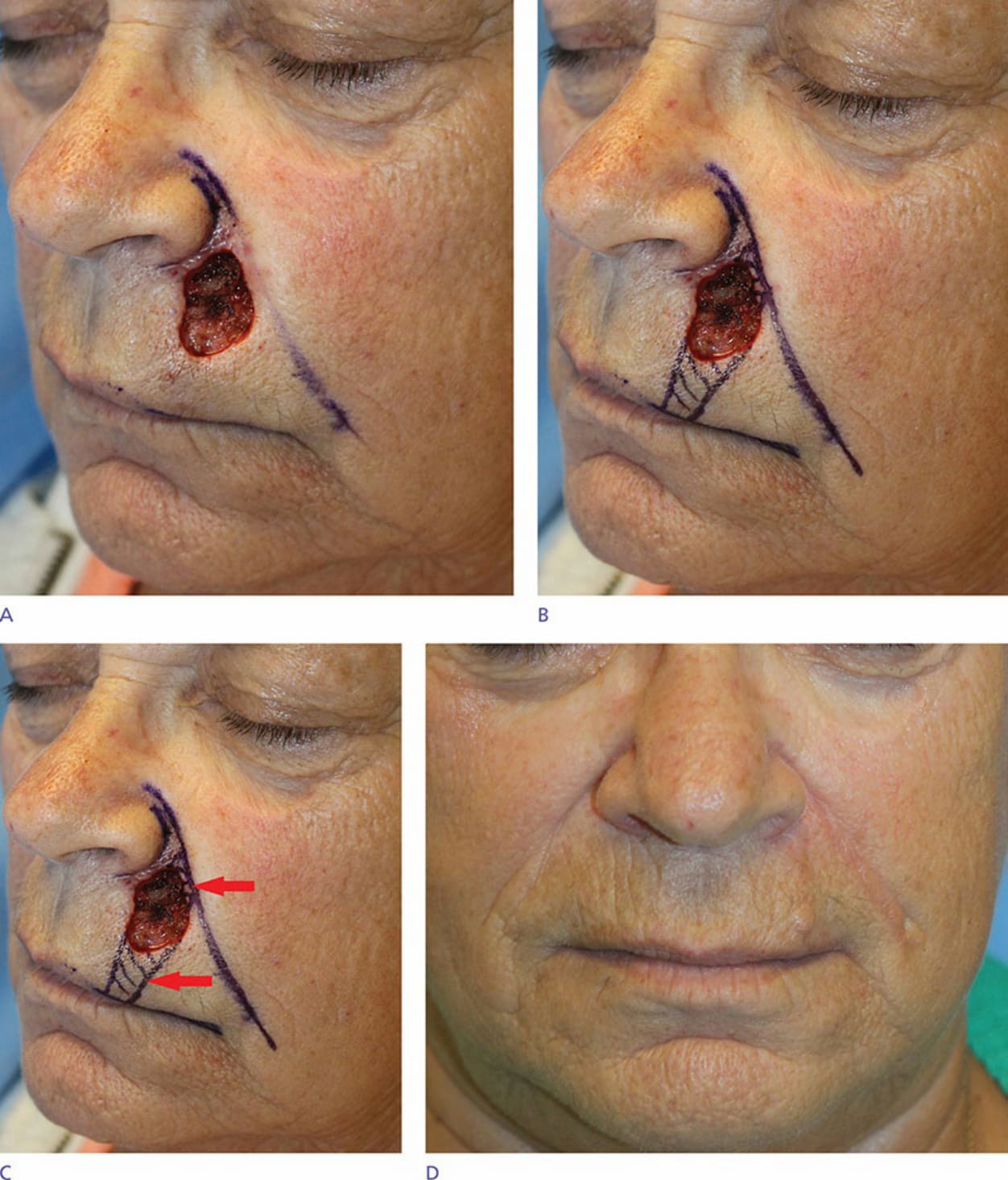
Figure 21-18. A defect on the left upper cutaneous lip resulted from removal of a squamous cell carcinoma with Mohs surgery (A). An O-to-U type advancement flap was designed with planned resection of the remainder of the lip cosmetic subunit (red arrows) between the nasolabial fold and the vermillion–cutaneous junction (B,C). Result at 2- week postop (D).