A-to-T flap
A-to-T flap
A frequently used technique, also known as an O-T advancement flap, the A-to-T advancement flap splits one standing cone into two smaller cones along the base of the flap (Figure 21-13). Often, the standing cone is at least partially sewn out by a “rule of halves” suturing technique (see Chapter 19) that may obviate the need for large displaced dog ears. This approach is frequently used on the forehead and lips. A stepby-step approach to this technique on a Mohs defect on the right upper lip, right philtral column, and nasal sill is shown in Figure 21-14.
either side of the peak of the vermillion-cutaneous junction below the right philtral column (C). The incisions for the advancement flaps were made along the nasal sill (D,E), and the flaps were undermined above the SMAS overlying the orbicularis oris (F,G). The wound was then closed in a layered fashion (H,I,J), and her 3-month postoperative result with preservation of free-margin position is shown (K).
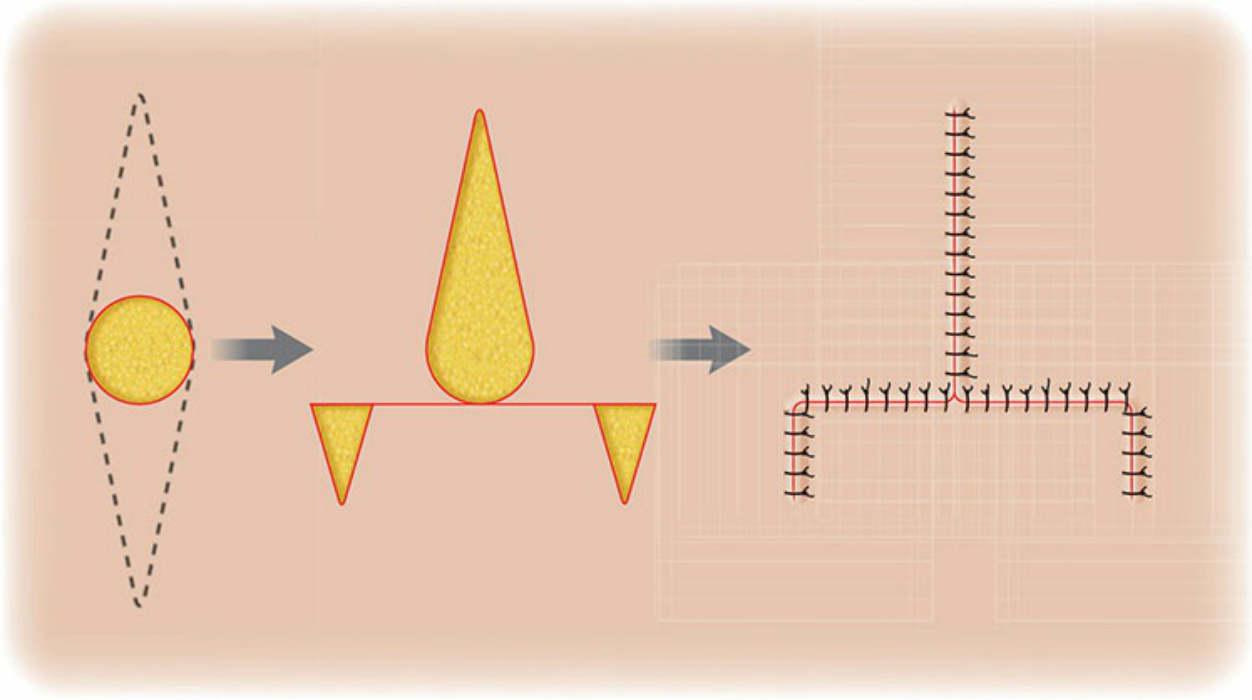
Figure 21-13. O-to-T flap design. Bidirectional primary tissue movement and one standing cone displaced.
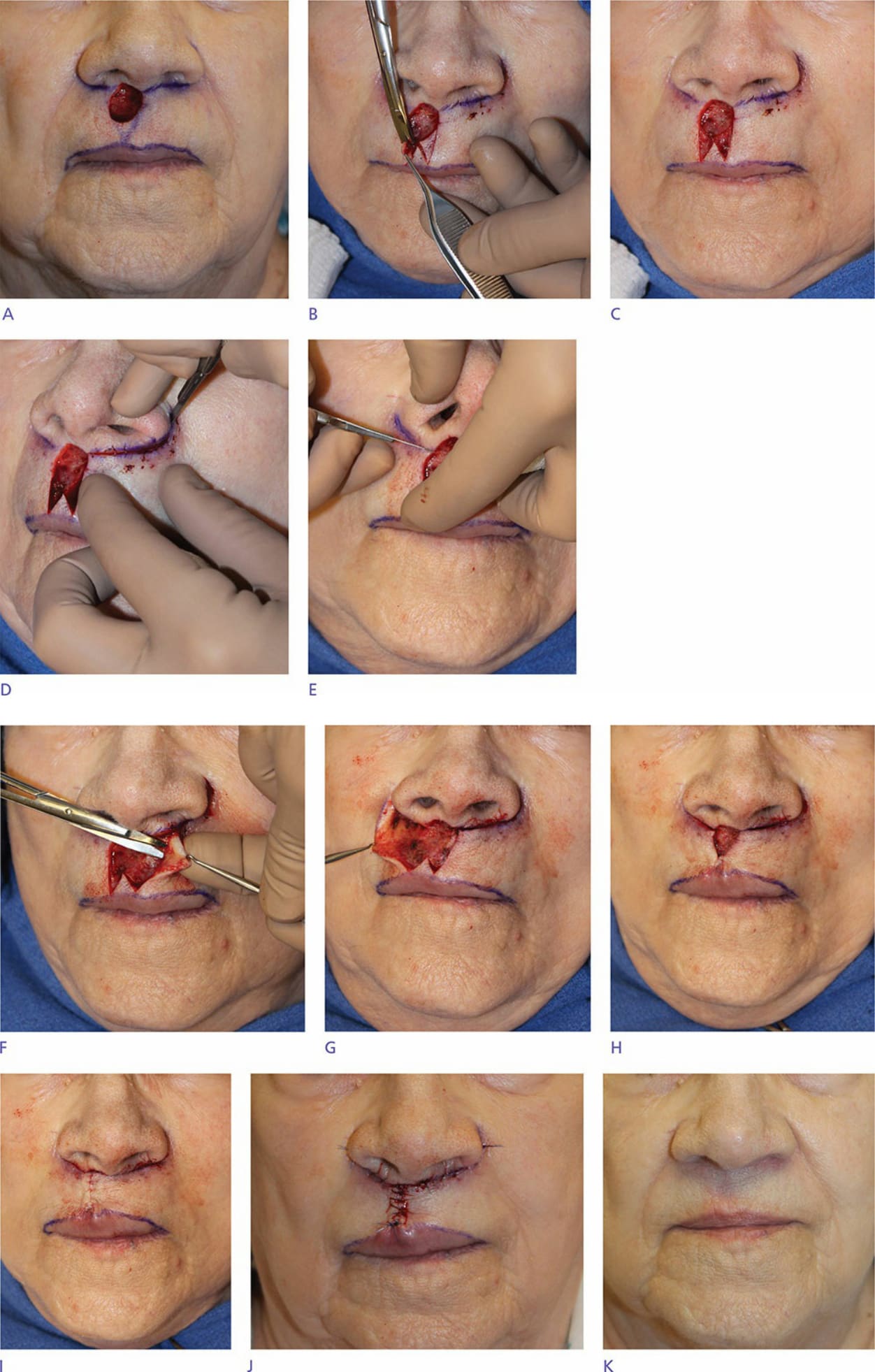
Figure 21-14. Defect after tumor removal (A). An O-to-T advancement flap with an M-plasty was designed to close the defect. First, the standing cones for the M-plasty were removed (B,C). The apices of the M-plasty were placed to