Flap vascularity
Flap vascularity
As discussed in detail in Chapter 20, flap survival depends on a reliable blood supply. The perfusion of blood through the vascular plexuses decreases as the distance from the feeding artery or arteriole increases. When the perfusion pressure is too weak to keep blood vessels patent, blood flow stops and necrosis ensues. The portions of an advancement flap most vulnerable to necrosis are the distal tip (since it has fewer blood vessels to nourish it and since it is most distant from the feeding artery or arteriole) and the portion of the flap sutured under the greatest tension (since the tension from the closure also results in compressive forces on blood vessels).
The ratio of the length of the flap to the width of its pedicle has a significant impact on perfusion. As a general guideline, random pattern flaps on the face can easily sustain a 3:1 length-to-width ratio, while those on the trunk and extremities may be best designed with a 2:1 ratio.4,5 These guidelines, however, are not absolute, as the robust facial blood supply may sustain flaps of significantly greater length-to-width ratios. Indeed, many flaps on the eyelid and helical rim6 are regularly executed with length-towidth ratios of 4:1 or greater. Moreover, at some point increasing the width of the flap pedicle fails to improve blood supply, as perfusion pressure may be insufficient to feed
an excessively long flap.7
The anatomic plane of flap elevation also impacts the flap’s vascular supply. Deeper undermining planes may incorporate larger caliber arteries with greater perfusion pressures, encouraging perfusion, though this must be weighed against the risk of damaging critical anatomic structures, such as branches of the facial nerve.
Ideal undermining planes for advancement flaps vary by anatomic location.8 For the majority of advancement flaps on the lateral face, the preferred anatomic plane is just above the SMAS, as this protects facial motor nerves, creates a flap of sufficient thickness to have a robust vascular pedicle, and permits clean and efficient flap elevation deep to the dermal and subcutaneous vascular plexuses (Fig. 21-5). On the central forehead, nose, and scalp, a sub-SMAS plane is usually preferred due to the relatively avascular nature of this tissue plane and the low risk for clinically relevant facial muscle weakness from cutting terminal motor nerve branches.
Wide flap undermining may decrease deep restraint, though it also may impair the blood supply by cutting vertically oriented perforating blood vessels that nourish the flap. Undermining should be performed carefully from the flap tip toward the pedicle only up to the point where sufficient movement is achieved. Additional undermining does not necessarily improve flap mobility because it does not influence the dominant restricting force of lateral restraint.9 Studies of tissue biomechanics have confirmed that wide undermining of advancement flaps does not add mechanical advantage or increase flap mobility.10
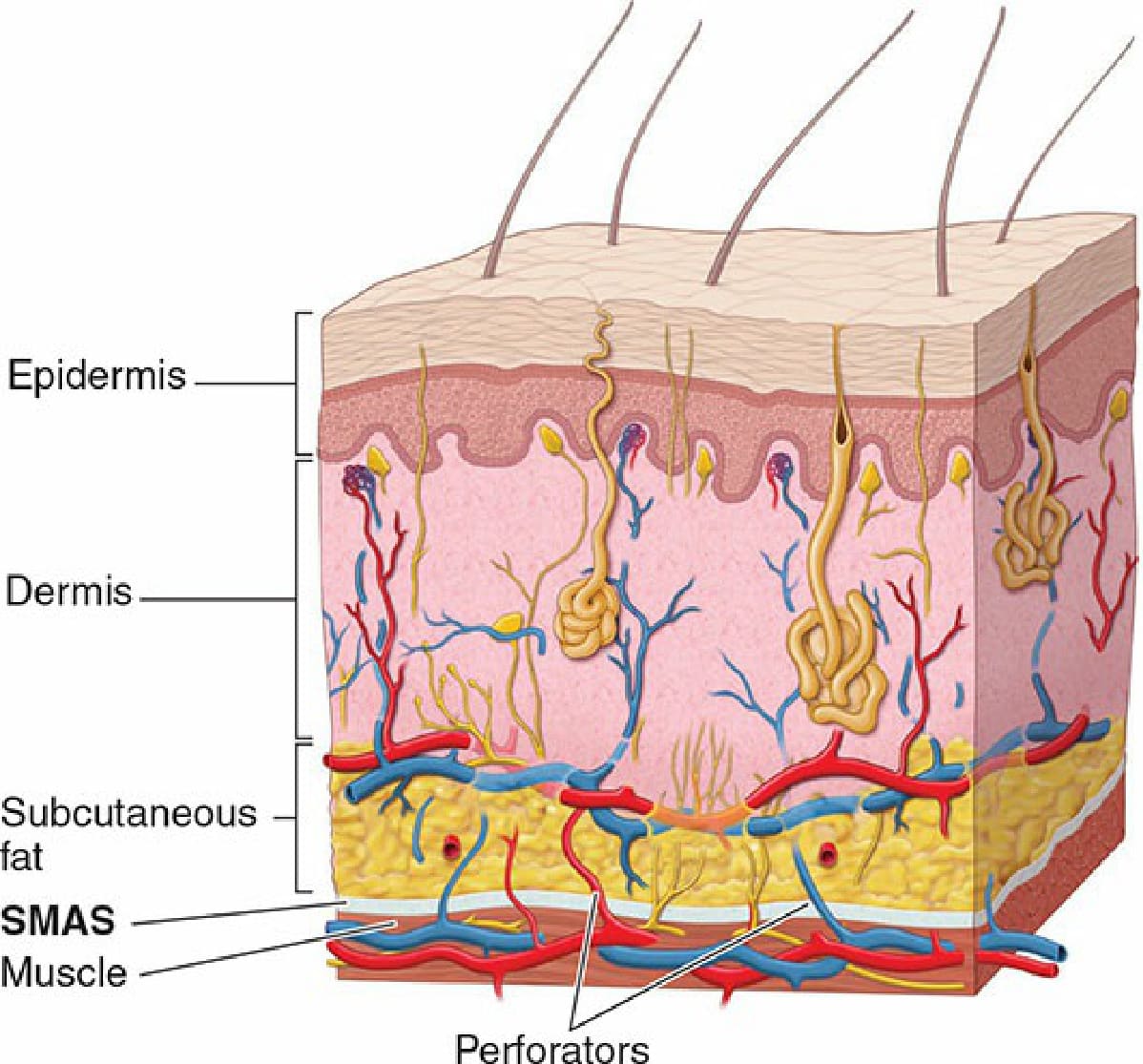
Figure 21-5. On the lateral face and neck, an undermining plane above the superficial musculoaponeurotic system (SMAS) preserves maximal flap vascularity while protecting facial motor nerves branches, which lie underneath the SMAS and innervate muscles from their lateral undersurface.