Tension vectors
Tension vectors
In contrast with rotation and transposition flaps, advancement flaps do not significantly alter the direction or magnitude of the primary tension vector for wound closure. The direction in which the flap slides toward the defect is considered the primary tissue motion, and the countermovement of the surrounding tissue to meet the flap is considered secondary tissue motion (Fig. 21-2). For defects of the midline face, the primary motion is usually lateral to medial; for defects of the lateral face, the primary motion is usually inferior to superior. Tension typically runs in a single vector along the direction of primary and secondary tissue motions, similar to what is seen with a linear closure.
The free margins of the eyelids, nose, lips, and ears are vulnerable to distortion from nearby advancement flaps.2 To avoid distortion of the anatomic landmarks, advancement flaps are usually designed to orient tension vectors parallel to the free margins. However, in some cases, it is preferable to design a flap so that the main tension vector
is oriented perpendicular to the free margin. Tacking sutures that anchor the undersurface of the flap to relatively immobile periosteum or the origins of underlying muscles may diminish or eliminate tension at the primary defect and prevent free-margin distortion. On the central face, superficial musculoaponeurotic system (SMAS) plication sutures may also decrease tension at the dermal edges of the primary defect.
The primary motion of the flap faces resistance from three main extrinsic forces: lateral restraint (whose vector runs opposite to the direction of primary motion), deep restraint from the host bed, and superior/inferior restraint of the adjoining skin tissue (Fig. 21-3).9 Lateral restraint causes the greatest restriction, and is dependent on the elasticity and mobility of the donor skin. Deep restraint from the host bed is the next most restrictive, and can be largely mitigated by undermining. Superior/inferior restraint is the least restrictive force, and may be diminished by extending the length of the flap as long as perfusion pressure remains intact. For a full discussion of flap dynamics, see Chapter 20.
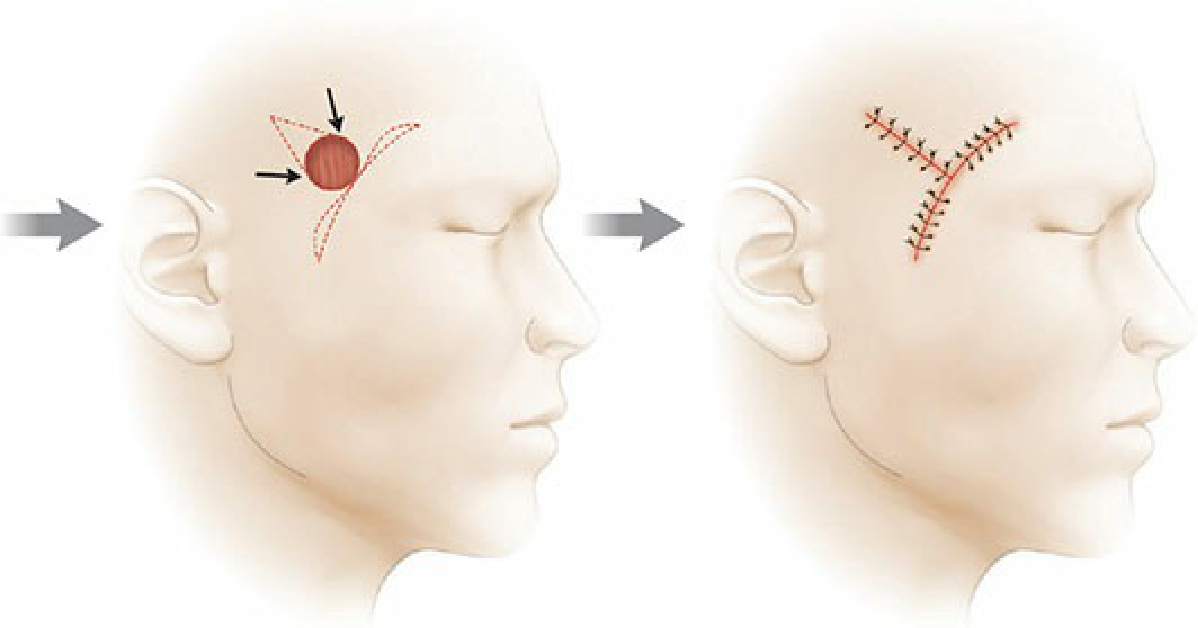
Figure 21-2. Closure with an advancement flap relies on the primary motion of the flap and the secondary motion of the surrounding tissue to meet the flap. Keeping the tension vector parallel to free margins helps to preserve their position.
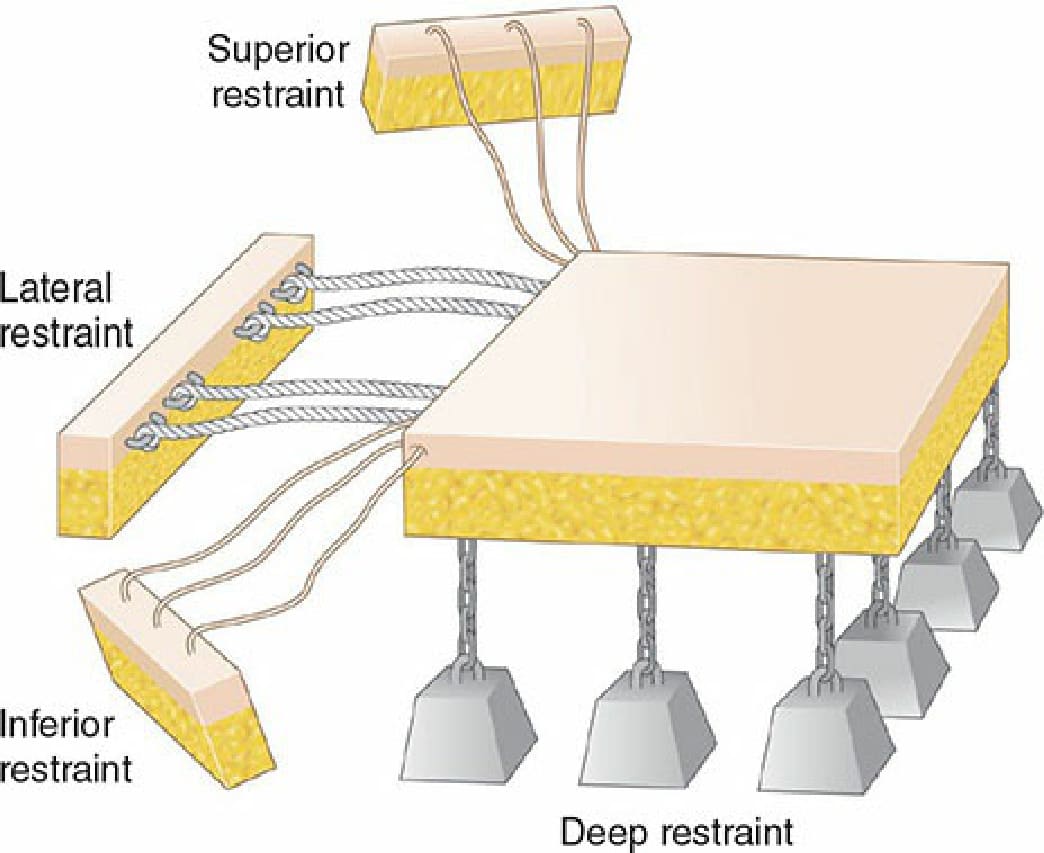
Figure 21-3. The resistance to flap advancement comes from three main extrinsic forces: lateral, deep, and superior/inferior restraint. Among these factors, lateral restraint directed 180 degrees away from the direction of flap advancement is of the greatest significance. Undermining largely mitigates deep restraint.