VASCULAR SUPPLY
VASCULAR SUPPLY
Adequate vascular supply of a flap is of paramount importance for flap survival. By definition, all flaps provide the vascular supply needed to provide the gas exchange and nutritional support required for their survival. The base or pedicle of the flap is the area that remains attached to the skin adjacent to the surgical defect and contains the source of this vascular supply. The tip of the flap is the portion of the flap furthest from the base, and is the portion of the flap that is most at risk for necrosis and failure secondary to insufficient blood supply.
Various ways to categorize cutaneous flaps exist; one such approach is to categorize flaps according to vascular supply. Using this classification system, the two main categories of cutaneous flaps are random and axial pattern flaps (Table 20-2). Random flaps include those that are supplied by unnamed arteries. In cutaneous surgery, there are a nearly infinite number of random flaps that can be designed on the face due to the abundant vascular supply and plentiful anastomoses. Blood supply of random flaps is derived from perforators of musculocutaneous arteries at the base of the flap, and delivered to the tip by the interconnecting vessels in the dermal and subdermal plexuses. Axial flaps, in contrast, are those that incorporate a named artery within their pedicle; this named septocutaneous or musculocutaneous artery runs within the long axis of the flap. When a flap extends beyond the reach of the named artery, the distal portion is functionally a random pattern extension of the axial pattern flap. In dermatologic surgery, the most commonly encountered axial flap is the paramedian forehead flap, deriving its blood supply from the supratrochlear artery.
In planning a cutaneous flap, various forces that affect end perfusion must be considered. Vascular perfusion pressure is the force of blood flow through a vessel; this force must be greater than the capillary resistance in order to maintain vessel patency. As expected, perfusion pressure decreases as the distance from the feeding vessel increases. If the distance becomes too great, perfusion pressure will fall below the critical closing pressure of the vessel, and necrosis will occur due to lack of blood supply.9 This inverse relationship between the distance from the feeding vessel and
perfusion pressure historically dictated that flap length:width ratios should be in the order of 3:1 to ensure adequate vascular supply. This theory was challenged by work performed by Stell in 1979 that showed that while viable flap length is dictated by the width of the base, there is an upper limit of length survival that cannot be increased by widening the base of the flap (Fig. 20-3).9–14
In addition to perfusion and closing pressures, tension exerted on the blood vessels with the movement of the flap must also be considered. In general, movement and blood supply work countercurrent of each other. Just as in a flexible rubber tube, when tissue is stretched in order to close the primary defect, tension on the vessels will result in narrowing and ultimately the closure of the lumen if tension becomes too great. While this is a fairly minor consideration on the head and neck where blood supply is abundant, it is a major consideration on the trunk and extremities and in irradiated or heavily scarred areas where blood supply may be more tenuous.
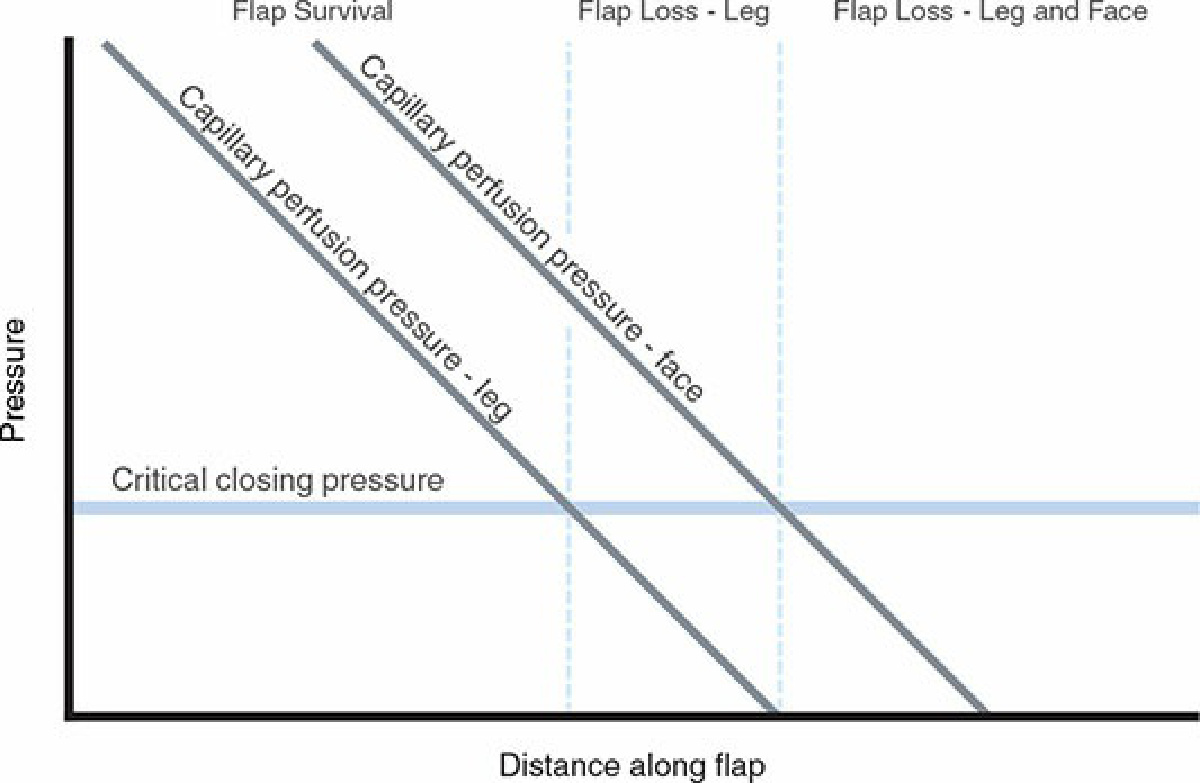
Figure 20-3. Flap perfusion and critical closing pressure. Perfusion pressure decreases as the distance from the artery and arterioles supplying the flap increases. Once capillary perfusion pressure falls below capillary resistance, blood flow ceases and distal flap necrosis occurs. Note the dependence on location, since areas with higher perfusion pressure, such as the face, are more forgiving.
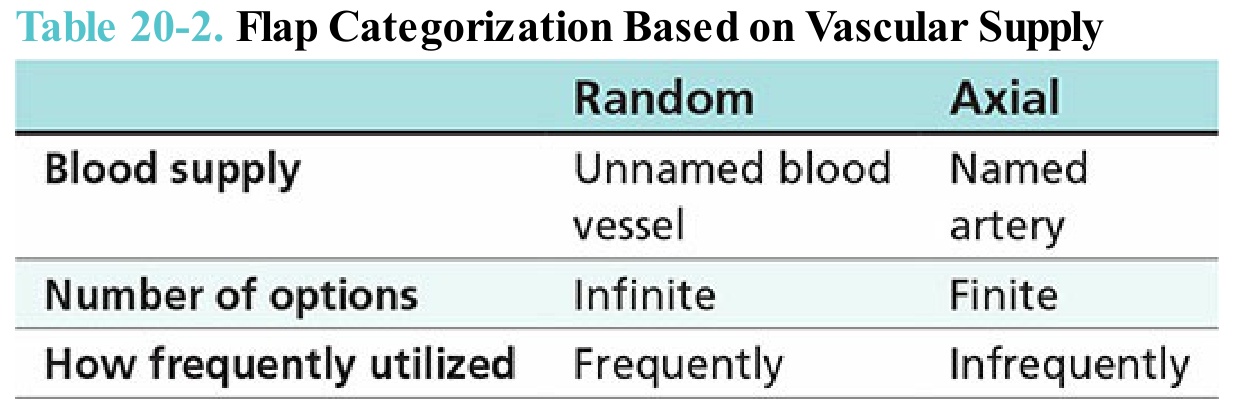
Table 20-2. Flap Categorization Based on Vascular Supply