NOMENCLATURE
NOMENCLATURE
The term “elliptical excision” has been used historically to denote linear wound closures, though numerous authors have, over the years, pointed out that the basic shape used by most dermatologic surgeons for closure design is not, in fact, an ellipse (Fig. 18-1).8–12 The term “fusiform excision” has, therefore, been proposed as an alternative, though it has yet to be universally adopted.
The rhombus, or tangent-to-circle, design is a geometrically efficient approach to linear wound closure. Note that rhomboid, however, does not mean rhombus-like, but rather refers a specific geometric shape defined by Euclid as a parallelogram where adjacent sides are of unequal lengths. Therefore, these closures should not, from a Euclidean perspective, be referred to as rhomboid.
Most linear excisions are closed in a layered fashion, with repair of the dermis and/or fascia preceding epidermal approximation. Surgeons may refer to an intermediate closure and complex closure; these terms relate to the billing of closures using CPT code series. As a general rule, extensive undermining, dog-ear correction, or other ostensibly complex steps are needed to bill for a complex closure.
Some surgeons refer to undermined flaps of tissue that are advanced into the center of a wound in order to close a linear excision. While it is technically appropriate to refer to undermined sections of tissue as skin flaps, no degree of undermining shifts a linear excision and repair to a bilateral advancement flap for billing purposes, as the latter requires a true adjacent tissue transfer (for a detailed discussion of flap dynamics and advancement flaps, see Chapters 20 and 21, respectively; for a discussion of billing, see Chapter 10).
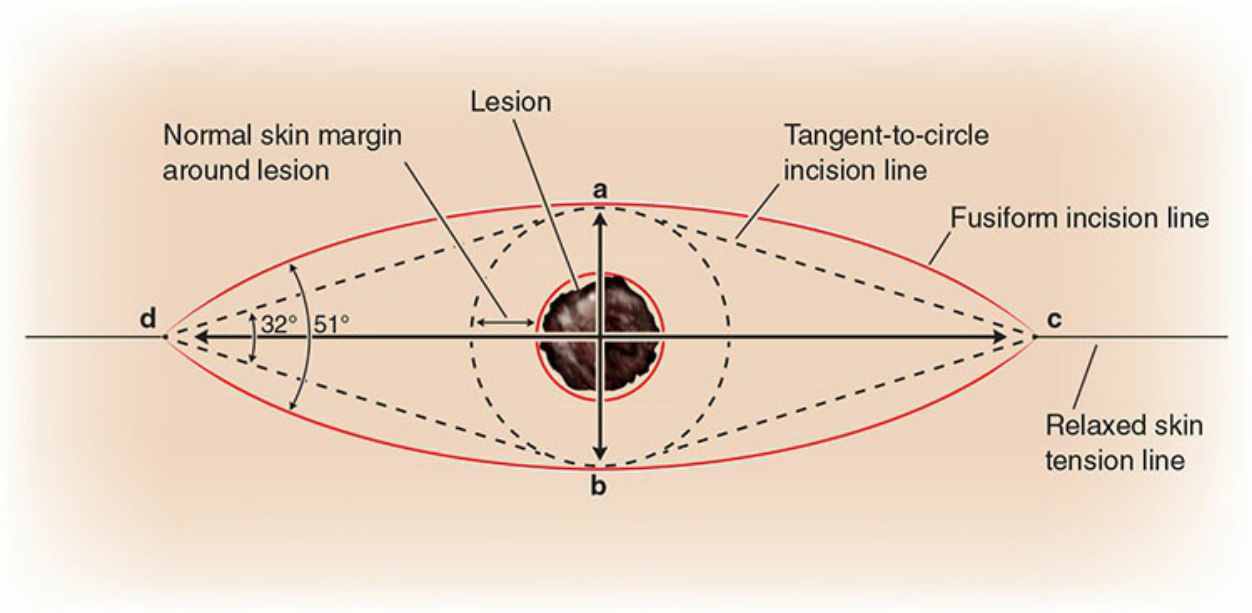
Figure 18-1. The rhombus (tangent to circle) closure inscribed within a fusiform design using a theoretical length-towidth ratio of 3.5:1.