DRAINAGE
DRAINAGE
Initially, the exudate may spontaneously drain after incision is performed secondary to built-up pressure. When the lesion is incised at the most fluctuant and dependent area, thin exudate will spontaneously drain out without the need to apply pressure to the lesion, as long as the incised area remains patent.
External pressure may be required in order to definitively drain the remaining exudate, though this may be at the expense of patient comfort. To minimize pain, it is important to apply pressure to the lesion carefully, though often the relief associated with internal pressure reduction outweighs ant transient pain associated with the placement of lateral pressure. Pressure is applied gently and slowly from the lateral
sides of the lesion toward the incision site (Figs. 17-1 to 17-5). Applying pressure from the top of the lesion at the incision site down to the bottom of the lesion may not result in effective drainage; indeed, the contents may move laterally toward the wall of the fluctuant mass when pressure is applied vertically, and this approach should therefore be avoided. For smaller masses, using a cotton-tipped applicator provides a better focal point of pressure than using a fingertip, which is much larger. If the patient experiences significant discomfort, additional injections of local anesthetic, possibly as a ring block, may be beneficial.
Curved hemostats may be used to enlarge the opening from a narrow slit-like space to a wider exit point, which is especially helpful for thick purulent exudate. The closed tips of curved hemostat clamps are inserted into the incised area and then opened to widen the incised area. The nondominant hand is used to apply pressure to further drain the contents. Hemostats may also be used for careful blunt dissection to break up loculations and facilitate further drainage. Forceps can be used to open the exit for drainage, though they provide only minimal leverage. Care should be taken not to overly stretch and traumatize the skin edges with hemostats or forceps, as this may affect the healing and ultimate cosmesis of the incision site.
When I&D is performed on an acute hematoma, its solidity requires a larger incision and external pressure to remove the clot. Older blood collections can be drained with a shorter incision length or an 18G needle. Attention should be paid to any fresh red blood when I&D is performed on hematoma, which may indicate active bleeding that would need to be definitively surgically addressed.
For acute paronychia with an abscess located immediately adjacent to the nail sulcus, the tip of a #11 or #15 surgical blade or 21G or 23G needle may be gently inserted underneath the proximal or lateral nail folds to create an opening for drainage.7,8 Gentle pressure is applied to extrude the purulent exudate. Care should be taken to point the sharp edge away from the nail, and not to insert it too aggressively in order to avoid damaging neurovascular bundles, tendons, or the nail matrix. A piece of gauze may be placed underneath the nail fold to allow continued drainage.9 For an
abscess not located immediately adjacent to the nail sulcus, incision is made directly over the abscess and/or in line with the lateral nail fold to decompress the abscess.10
If indicated, swab culture and sensitivities may be sent out using freshly drained exudate. Avoid contacting the tip of swab with skin or mucosal surface to prevent contamination by normal flora. A sterile syringe may be used to obtain a sample from the interior aspect of the cavity.
Irrigation may be performed to further remove the infectious or inflammatory exudate. The tip of a sterile, normal saline-filled syringe is inserted through the incised wound, and the cavity is gently rinsed to thoroughly irrigate the cavity until the effluent is clear. Copious quantities of gauze or absorbent pads should be placed at the site to absorb fluid and minimize splash-back over the surrounding area and operator. The nondominant hand may be used to apply gauze to cover the incised area during irrigation. A syringe with a built-in splash shield may also be used. An appropriate incision size will enhance irrigation and prevent excessive buildup of pressure within the lesion.
If further drainage is required, wound-packing material, such as 1/4- or 1/2-inch packing strips with or without iodoform, is gently inserted through the incision site and loosely packed inside the lesional cavity using hemostats or forceps. This will prevent premature closure of the incised wound, which can lead to recollection. Care should be taken to avoid overpacking the wound, which could cause ischemia of the surrounding tissues and impede the desired drainage.11
Electrodesiccation may be performed after I&D of mucoceles or digital mucous cysts to close the dead space and avoid recollection of the exudate.12 Any active bleeding points are cauterized.
A pressure dressing may be needed on some lesions in order to collapse the cavity, minimize recollection of exudate, and minimize dead space, which could lead to reaccumulation. Dissecting cellulitis of the scalp requires pressure dressings and head wraps, as the exudate can rapidly reaccumulate. This pressure dressing may also serve to help control bleeding.
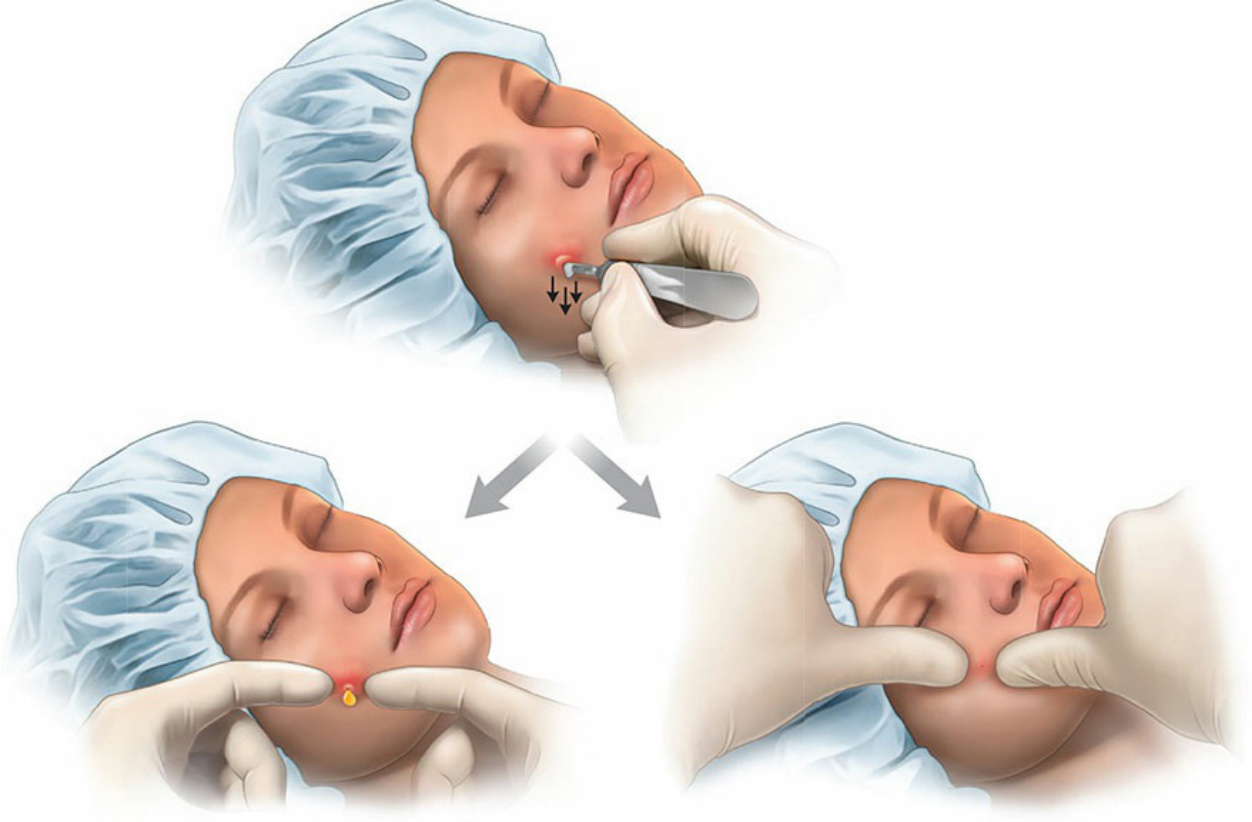
Figure 17-1. I&D on the most dependent portion of a cyst on a patient’s cheek in supine position utilizing gravity effect for the ease of drainage. Note that lateral pressure left) results in the extrusion of the contents, while downward pressure right) does not.
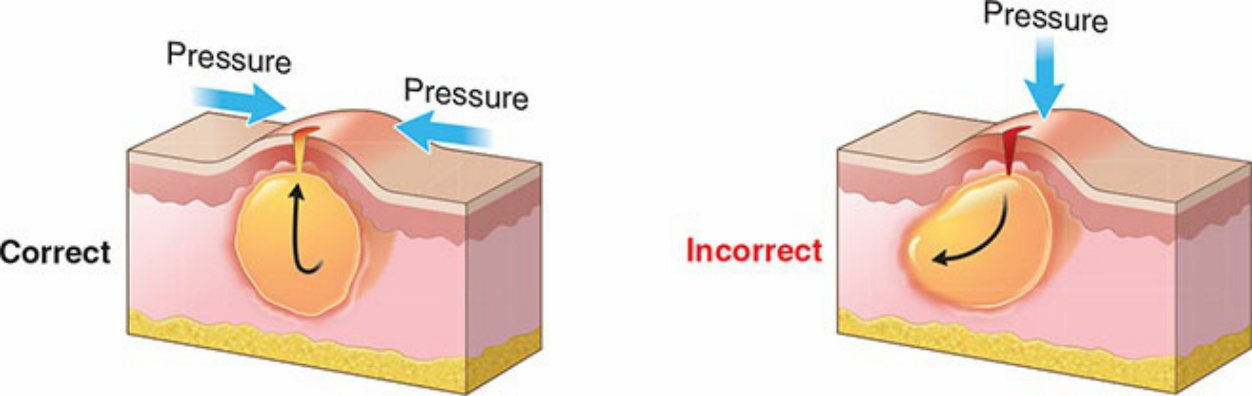
Figure 17-2. Pressure is applied gently and slowly from the lateral side of lesion toward the incision site, which moves the contents toward the exit provided by the incision. The contents may move laterally toward the wall of lesion and away from the exit when pressure is applied vertically.

Figure 17-3. A small stab incision is made at the inferior pole of the abscess.

Figure 17-4. Gentle lateral pressure is used initially to ensure that contents are effectively extruding through the incision.

Figure 17-5. Firm lateral and upward pressure is applied to force the expulsion of all cyst contents.