Introduction
CHAPTER 17 Incision and Drainage
Sirunya Silapunt Michael R. Migden
SUMMARY
I&D may be used to treat various conditions that require the release of enclosed
contents, such as hematomas, furuncles, and infected cysts.
Placing the incision parallel to relaxed skin tension lines may mitigate the
appearance of more prominent scars.
While these procedures are straightforward and can be performed with great
rapidity, a poorly performed I&D procedure may serve only to exacerbate an already unpleasant or even dangerous condition.
Beginner Tips
Choose the most fluctuant area of the lesion, which represents the most liquefied
portion of exudate, for easily drainage.
Choosing the dependent area to facilitate drainage by gravity effect may also reduce
the need for manual pressure and attendant patient discomfort.
Thicker exudate such as blood, coagulum, or mucin requires a longer time to start
draining.
Expert Tips
An 18G needle can be useful for I&D on very small lesions. Due to the small opening
of this type of incision, thick exudate may not drain out easily. After stabbing, keep the tip of the 18G inside the lesion, push the needle tip laterally to widen the slit-like cut, and wait for exudate to drain.
Collect fresh, uncontaminated exudate for swab culture to improve the accuracy of
culture and sensitivity; avoid collecting the skin surface–contaminated exudate. Allow the exudate to be collected to drain without running on the skin by compressing the lesion and holding the tip of the swab at the proper position and angle.
Don’t Forget!
If no or minimal drainage occurs, assess the patency of the incision site.
Inject lidocaine in the superficial dermis, not into the lesional cavity. Pain with
incision may occur when lidocaine injection occurs inside the lesion instead of the dermis and adjacent subcutaneous tissue. A ring block can also be considered.
Pitfalls and Cautions
The incision should be stopped as soon as the surgeon senses low tissue resistance, in
order to avoid tissue damage at the base of lesion.
Bleeding at incision sites is common. Use external compression to control bleeding.
Patient Education Points
I&D is a fast and effective procedure, but does not guarantee that a given fluid
collection will not recur.
For inflamed or infected cysts, patients should be warned to expect recurrence, and
definitive excisional surgery may be needed in the future.
I&D requires significant postoperative care, as wounds generally need to be packed or
cared for in other ways. Patients should understand that postprocedure management is a process, and drainage may persist for longer than anticipated.
Billing Pearls
I&D of an abscess is most frequently coded using CPT code 10060. When draining
multiple abscesses, 10061 may be coded, and this code may be used for “complicated” lesions as well, though its use should clearly be justified in the body of the surgical report. Additionally, 10140 may be used for nonabscess I&D. The 10160 code may be more appropriate when performing I&D using an 18G needle alone.
CHAPTER 17 Incision and Drainage
INTRODUCTION
Incision and drainage (I&D) is commonly performed in both general and procedural dermatology outpatient settings. This approach may be utilized to treat various conditions that require the release of enclosed contents, such as hematomas, furuncles, infected cysts, and collections of other extraneous substances. While the advantage of I&D is that it is easy to perform, patients should be warned regarding the requirement of postprocedural care. Moreover, since expression of the entire cyst wall is rarely effected when treating inflamed or infected cysts, recurrence of such lesions may be seen (Tables 17-1 and 17-2).
There are no absolute contraindications for I&D. Abscesses of the palms and soles can be associated with complications, and may require consultation with an appropriate surgical specialist. In select cases, I&D may be best performed in an operating room with conscious sedation. These include extremely large abscesses, complicated skin and soft tissue infection involving deeper invasion of tissue, or deep abscesses in areas that are difficult to anesthetize.
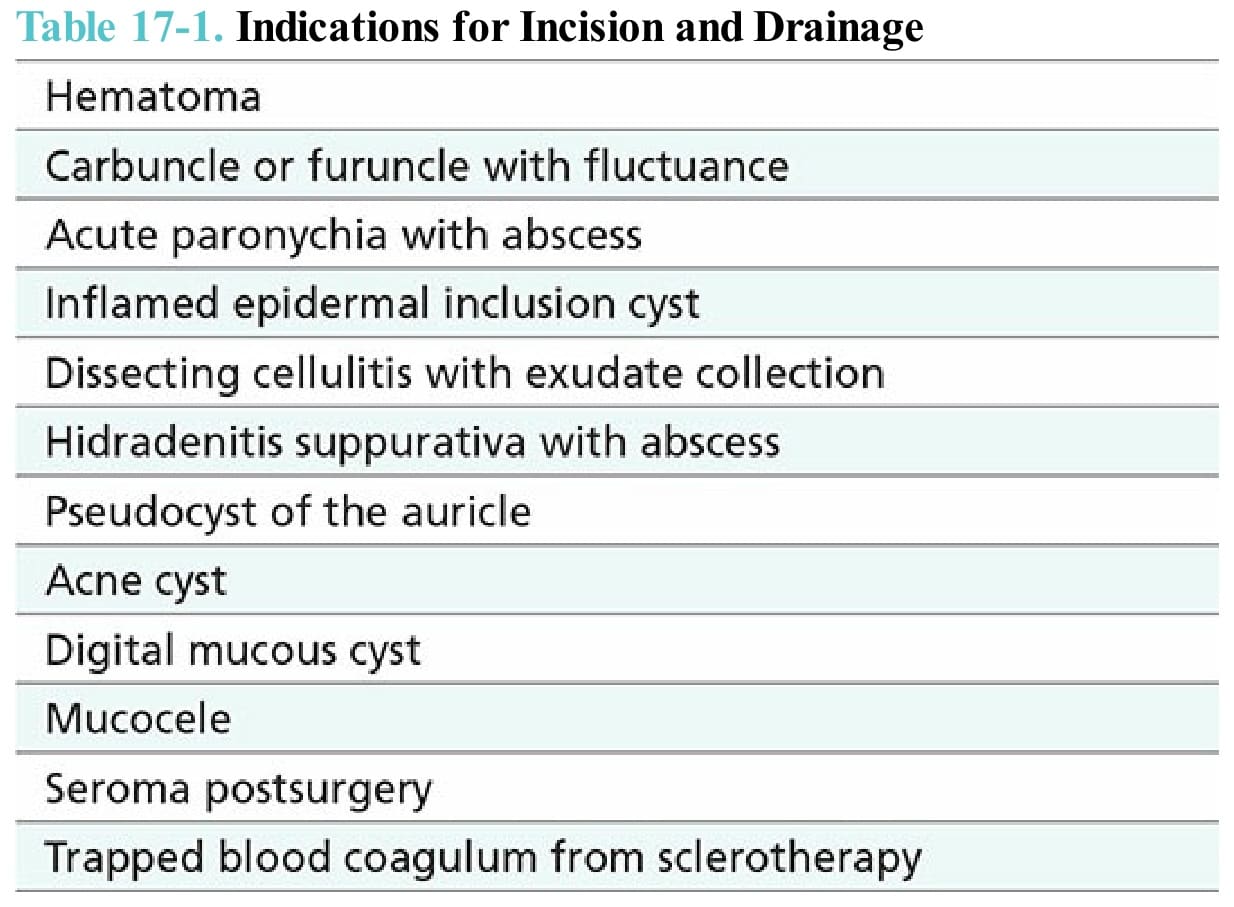
Table 17-1. Indications for Incision and Drainage
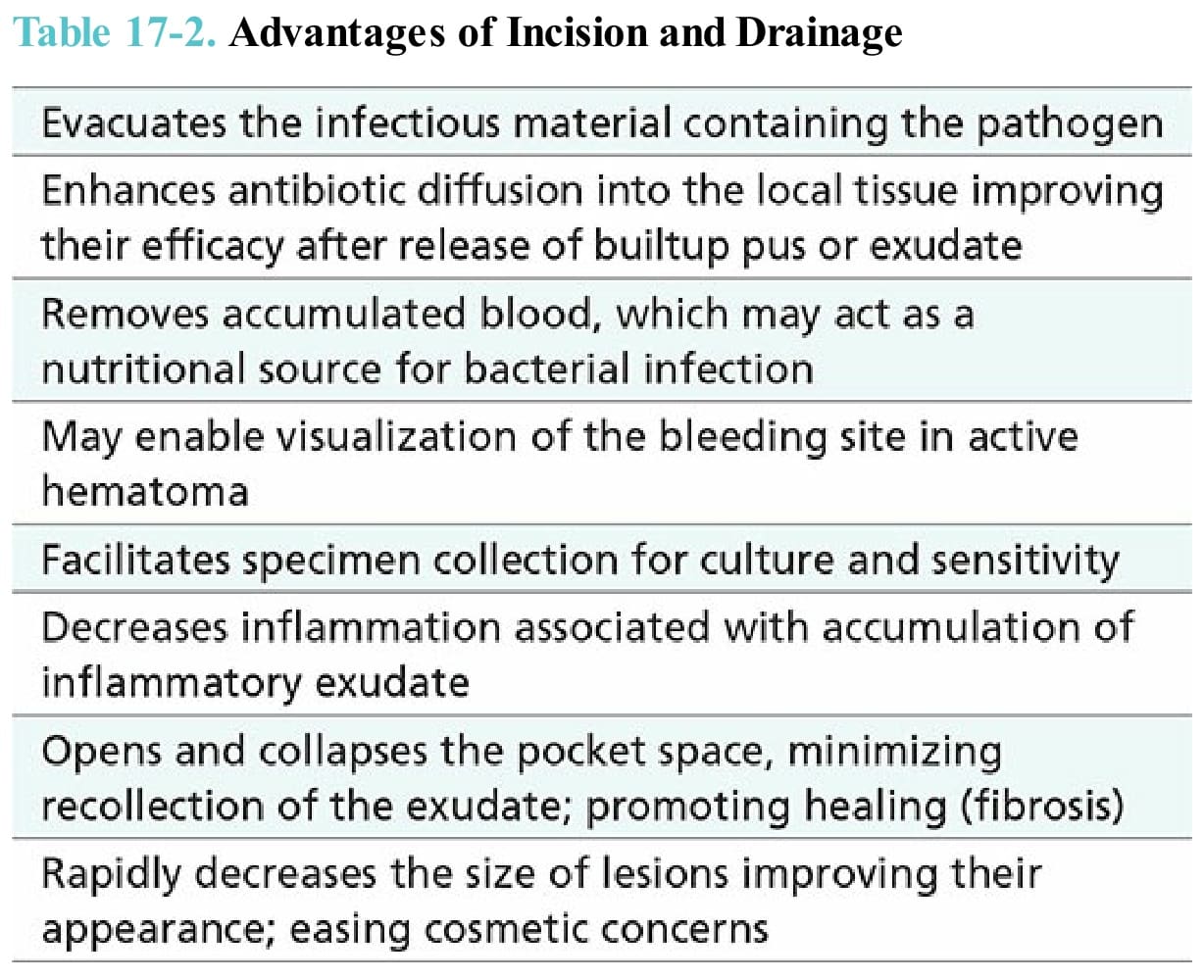
Table 17-2. Advantages of Incision and Drainage