TECHNIQUES
TECHNIQUES
While there are no absolute contraindications to cryosurgery, some comorbidities are more likely to be associated with adverse outcomes. Some of these include known cold intolerance, cold urticaria, cryofibrinogenemia, cryoglobulinemia, and Raynaud’s phenomenon. Collagen vascular disease, multiple myeloma, hemodialysis, thrombocytopenia, agammaglobulinemia, and blood dyscrasias of unknown origin have also been noted as relative contraindications.9
Several factors affect the amount of tissue destruction achieved with cryosurgery. When tissue is frozen, an ice ball forms that serves as a visible indication of the extent of surface freezing (Fig. 15-3). However, the depth of freezing, also referred to as the depth dose, may be more difficult to determine. The ice ball maintains a hemispherical shape until it reaches a depth of 5 to 7 mm, at which point it will begin to plateau. For lesions exceeding this depth, a thermocouple may be useful. This device should be inserted into the skin at a 25- to 30-degree angle until the tip reaches the base of the lesion, and will provide a more accurate determination of tissue temperature, though these are rarely used in clinical practice.
The temperature achieved with cryosurgery is directly related to the degree of resultant cellular injury. Melanocytes are most sensitive to cold, and are irreversibly damaged at temperatures ranging from −4° to −7°C. Keratinocytes are destroyed at temperatures ranging from −20° to −30°C, and death of fibroblasts occurs between −30° and −35°C. Malignant cells are most resistant to cold-induced damage, requiring
temperatures below −40°C for destruction.10 Therefore, when treating a malignancy, a temperature endpoint between −50° and −60°C is advisable (Fig. 15-4).
The freeze time, or duration of cooling, is another important consideration. In general, benign lesions require shorter freeze times, and may be sufficiently treated with a single freeze–thaw cycle. Malignancies often require a double freeze–thaw cycle, and freeze times exceeding 45 seconds.
Additionally, the lateral spread of freeze, or margin of freeze, varies depending on the type of lesion. For benign lesions, margins of 2 to 3 mm are sufficient, whereas malignant lesions may require margins of 5 mm or more.
Certain adverse responses, such as pain and blistering, should be anticipated following cryotherapy; when these become intolerable or progress to longer-term effects, they may be considered complications.
In the absence of local anesthetic or pre-existing neuropathy, all patients will feel pain during the treatment. Many patients will describe burning or stinging pain initially that may progress to a dull throbbing pain. The pain usually resolves spontaneously within minutes. Treatments to certain parts of the body, such as the ear, finger tips, lips, temples, and scalp may cause more severe pain. Additionally, cryosurgery to the scalp, temple, or forehead may occasionally be associated with migraine-like headaches.9
Almost all treated patients will also develop localized edema, blister formation, and erythema (Fig. 15-5). The amount of edema is related to both the intensity of the treatment and the lesion location. The eyelids, labia minora, lips, and foreskin have
more lax skin and therefore develop greater edema.9
Hypopigmentation is perhaps the most common complication. One prospective study of 421 actinic keratoses treated with cryosurgery reported hypopigmentation in 29%. The incidence of hypopigmentation increased with the duration of freezing time.11 This
may stem mechanistically from the fact that melanocytes are more cold-sensitive than keratinocytes and fibroblasts. Hypopigmentation is especially common in those with darker skin types. Paradoxically, hyperpigmentation may also develop following cryosurgery-induced inflammation.
Sensory and motor neuropathy may also develop following cryosurgery. The extent of neuropathy will depend on the cryosurgery dose and lesion location. One study of sensory neuropathy associated with cryotherapy revealed complete recovery in all subjects by 18 months.12 Infection, atrophy, hemorrhage, milia, hypertrophic scarring, bone necrosis, ectropion, and alopecia are additional reported complications.9

Figure 15-3. When tissue is frozen, an ice ball forms that serves as a visible indication of the extent of surface freezing.
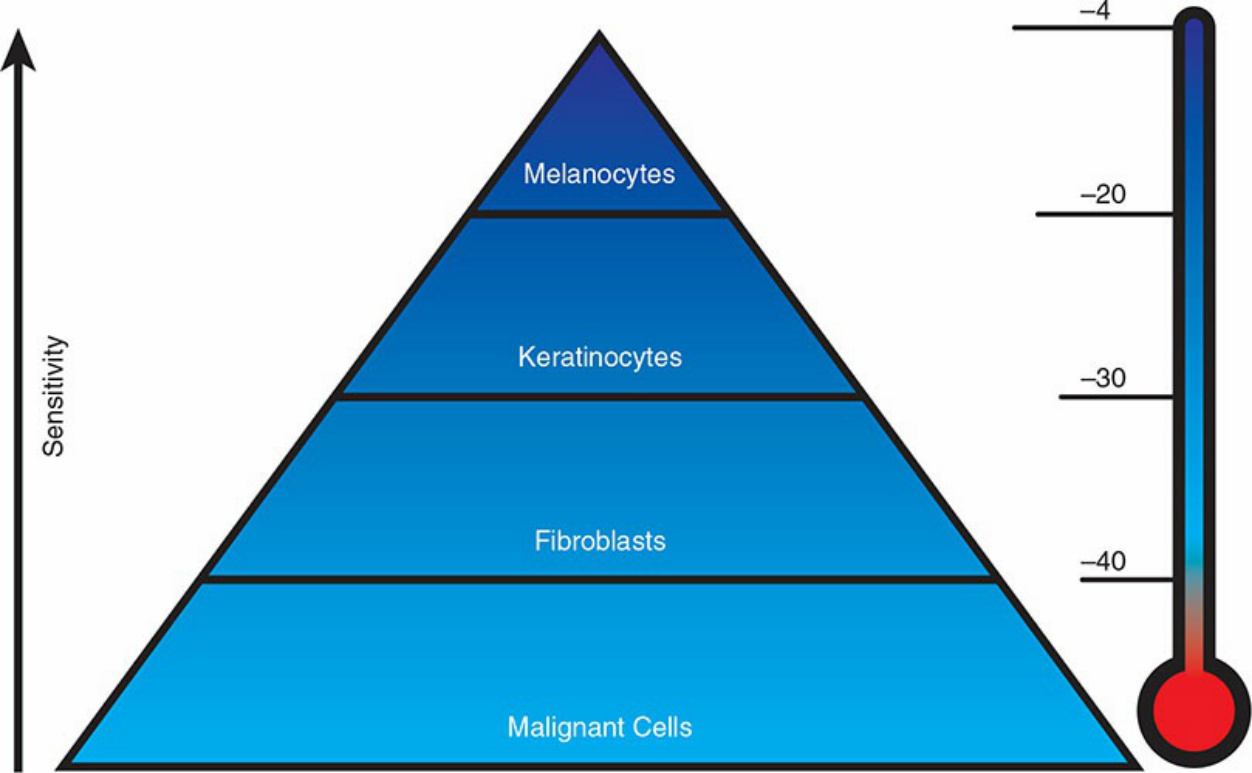
Figure 15-4. There is marked variability in the cold sensitivity of different cell types.

Figure 15-5. Almost all treated patients will also develop localized edema, blister formation, and erythema. Note the immediate postprocedure erythema.