Punch
Punch
The punch technique can be used to sample an inflammatory process, a lesion, or for complete excision of a smaller lesion. Furthermore, lesions slightly larger than 4 mm can often be forced into a 4-mm punch, resulting in satisfactory removal or sampling and a smaller wound.
The technique. When possible, the skin is pulled taught perpendicular to the skin tension lines, so that the wound created by the punch is oval and aligned with the preferred lines of closure. The punch is twisted gently (Fig. 14-5) until the full thickness of the metal portion has entered the skin (Fig. 14-6). The resulting specimen should be removed gently with a needle or by grasping the skin edge with toothed forceps to avoid crushing the specimen (Fig. 14-7). The resulting defect should then be assessed for the ideal closure vector (Fig. 14-8). A suture is placed (Fig. 14-9) and the wound may be closed with either a simple interrupted suture or a cruciate mattress suture (Fig. 14-10). Other novel punch biopsy devices are available as well.7

Figure 14-5. The punch is twisted gently.

Figure 14-6. This continues until the entire device is inserted (when working on the trunk) or once the deep fat has been entered, as seen here.
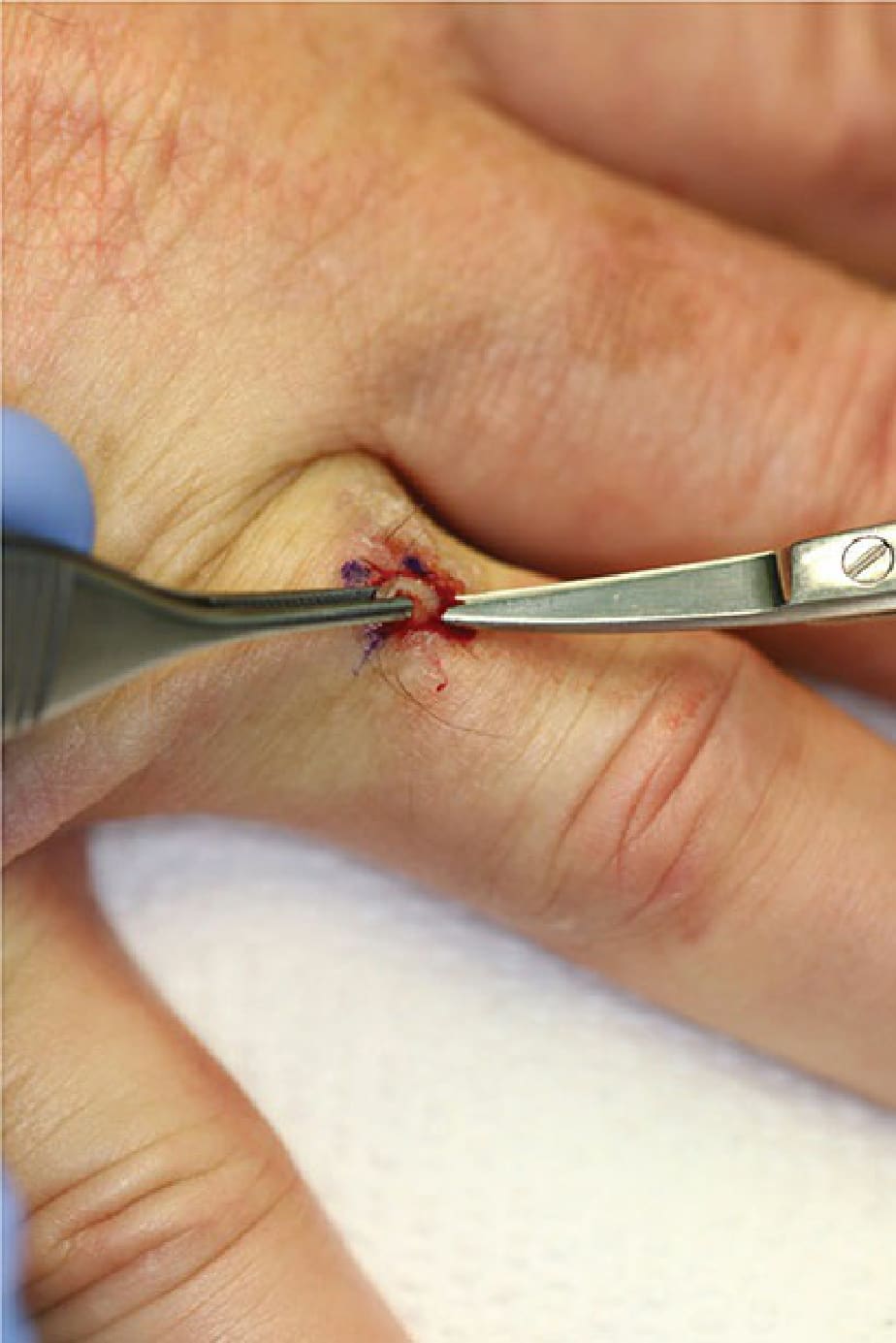
Figure 14-7. The specimen is grasped with forceps, elevated, and the base is snipped if needed at the level of the deep fat.

Figure 14-8. The resulting oval defect should be assessed for the ideal closure vector.

Figure 14-9. A suture is placed.

Figure 14-10. The cruciate mattress suture, essentially two throws of a simple running suture, is useful for punch biopsy closures.