ANTIBIOTIC SELECTION
ANTIBIOTIC SELECTION
In regard to the selection of antibiotics, guidelines are generally derived from the internal medicine and surgery literature, as there are few randomized double-blind studies for antibiotics in dermatologic surgery.11 The choice of antibiotic use in dermatologic surgery is shown in Table 7-7. Cephalexin and dicloxacillin are systemic agents used for prophylaxis on nonmucosal surfaces to cover gram- positive and gramnegative bacteria. Per AHA guideline, S. viridans and Peptostreptococci can be treated with amoxicillin. For perineal skin, amoxicillin–clavulanate can be selected to combat potential penicillin-resistant organisms. For Pseudomonas, fluoroquinolones such as ciprofloxacin can be used. If a culture is obtainable, antibiotics can be selected based on antibiotic sensitivities. Otherwise, antibiotic use can be tailored to the bacteria most commonly found in the local population, the patient risk factors, the surgical site risk factors, and the surgical risk factors.
An Advisory Statement has recommended antibiotic therapy based on the procedure type and anatomical location as well as patient allergies to penicillin or inability to tolerate oral antibiotics (Table 7-7).36 Cephalexin or dicloxacillin can be used as prophylaxis for wedge excisions of the lip or ear, flaps on the nose, and grafts. For those with penicillin allergy, clindamycin or azithromycin can be used, and TMP-SMX or levofloxacin may be used for anatomical sites in the groin or lower extremities. For patients who are unable to tolerate oral antibiotics, parenteral antibiotic therapy can be used. Lastly, for patients who are unable to tolerate oral antibiotics and who have a penicillin allergy, clindamycin can be used and gentamicin added to cover for the possibility of P. aeruginosa infection in the groin or lower extremities.36
Antibiotics are typically given the hour before the procedure. It is thought that this time permits the antibiotic to travel to the surgical site. Parenteral antibiotics are typically given half an hour preprocedure. However, there is ambiguous data about whether prophylactic antibiotic timing affects the risk of SSI.45 For longer procedures, the desired duration of action of the antibiotic should be considered. Blood can neutralize some antiseptics as well. For carriers of S. aureus, transient decolonization of S. aureus from the nasal area can significantly reduce the infection rate, and the use of topical mupirocin–chlorhexidine reduces the infection rate by half.24,46
For SSI, wound culture, microscopy, and antibiotic sensitivities should ideally be performed, and antibiotics should be tailored based on the sensitivities.
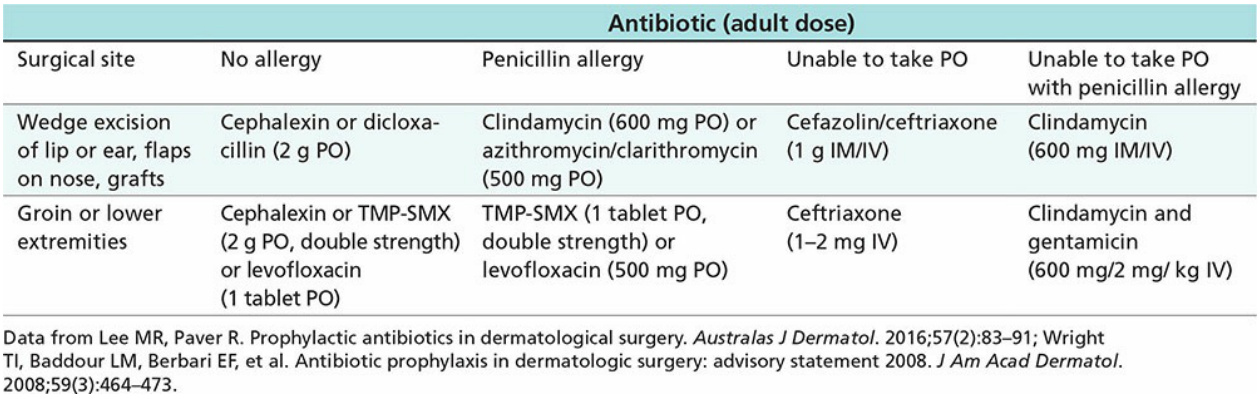
Table 7-7. Choice of Antibiotics for Prophylaxis in Patients at Risk of Surgical Site Infection