PREOPERATIVE EVALUATION
PREOPERATIVE EVALUATION
The preoperative evaluation is most simply thought of as an evaluation of the physical, medical, and emotional preparedness of the patient for a selected procedure. This formal evaluation is generally a multifaceted discussion regarding the procedure; a review of the patient’s history, medications, and allergies; any appropriate physical examination; obtaining informed consent through a process; and answering patient and/or family questions. The evaluation can be performed up to several weeks in advance of the surgery, though it may also take place on the same day of the procedure. If a same-day evaluation is chosen, the physician must be prepared to cancel the procedure if it is discovered the operation scheduled is inappropriate for the lesion, or the patient is not a good surgical candidate for medical or psychological reasons. There
are many factors that should be taken into account when deciding upon the timing of this evaluation including office setup, physician preference, patient mobility, and travel distance. Nevertheless, the preoperative evaluation ultimately serves as a forum to assess probability of overall success and cement the patient–physician relationship.
Team care is a critical component of the preoperative evaluation. It begins with the very first patient contact and continues up to the initiation of the procedure itself. All members of the team should be empowered and encouraged to have input in this evaluation and have the authority to halt it for any concerns. From the first moment the patient steps into the office, the front office staff has the opportunity to begin collecting information, such as the patient’s mood and degree of anxiety. The medical assistants and nursing staff carry this process forward, with obtaining a history, complete medication list, and any other standard data points necessary for the field of practice.
Certain subtleties become evident over time, such as personality, forgetfulness, unrealistic expectations, or specific fears that can be noted by the staff and guide the remainder of the visit. These observations can be acted upon early and preemptively, helping to tailor the patient care experience in a positive fashion. Moreover, these initial encounters should serve as a filter for red flags like abnormal labs or vital signs, concerning new symptoms, or patient aggression/combativeness. Safety is the responsibility of the team, and the surgeon, as team leader, must use all information gathered to determine the safest way forward. Overall, the guiding principle is that every person of the care team plays an essential role in the overall patient evaluation and experience. Table 3-1 is a summary of possible reasons for delaying a procedure.
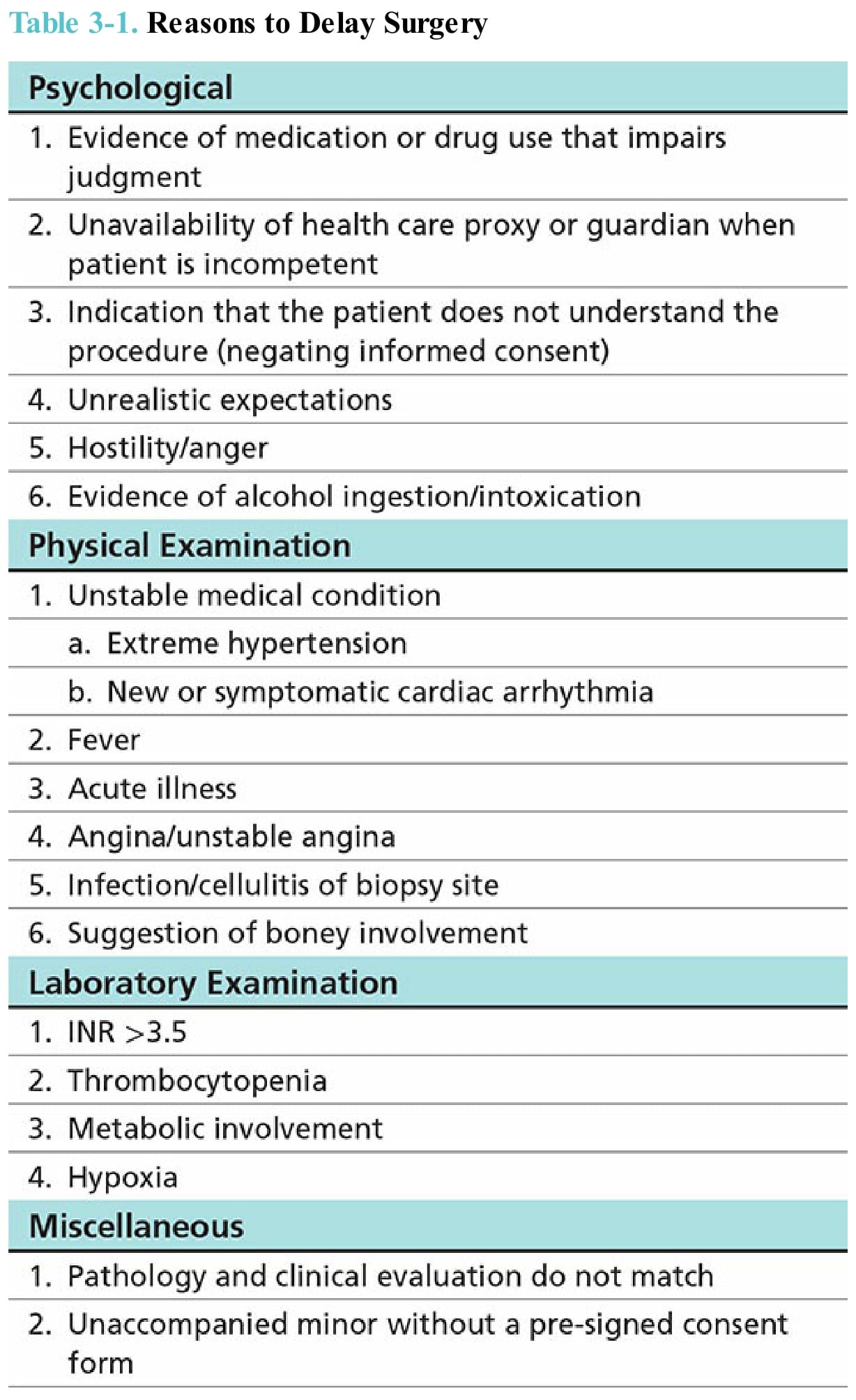
Table 3-1. Reasons to Delay Surgery