Cheek
Cheek
The anterior region includes the buccinator muscle, buccal fat pad, buccal
branches of the facial nerve, and the downward traversing parotid duct.
The parotid region is dominated by the parotid gland and underlying deep masseter
muscle.
The parotid duct and facial artery are easily identifiable landmarks in this region.
The marginal mandibular nerve is a key structure in the mandibular region as it
consistently crosses the facial artery deep to the fibers of platysma.
Anatomically, the cheek extends from the anterior border of the ear, limited medially by the nose, lips, and chin, and from the mandible up to the zygomatic arch and orbital rim. However, to best appreciate the cosmetic unit of the cheek, it is best described in three regions: the anterior, mandibular, and masseter–parotid regions.4,9,22
The anterior region contains many of the muscles of facial expression. The risorius is very superficial and of variable size, sometimes even absent. The zygomaticus major and minor as well as the levator labii superioris and the levator labii superioris alaeque nasi originate from the zygomatic bone and orbital rim, and are overlapped by the fibers of the orbicularis oculi muscle. When reflecting the skin over this region, zygomaticus minor is seen more superficially than the rest of the muscles, with only a few millimeters of subcutaneous tissue overlying it (Figs. 1-6 and 1-23). Since the facial nerve branches maintain their course and innervation deep to the muscles, injury to these branches is less likely provided that the plane of dissection remains superficial to the muscle plane.
Along the medial aspect of the anterior cheek, the facial artery can be seen anterior to the facial vein after crossing the mandible to ascend toward the angle of the mouth where it gives off the labial branches and subsequently traverses the nasolabial grove as the angular artery. Within the nasolabial groove, the angular artery can be accessed with little difficulty by dissecting within the subcutaneous tissue and overlying muscle slips of the zygomaticus major and minor muscles (Fig. 1-19). The angular artery then terminates at the medial canthus just above the medial canthal tendon by anastomosing with the ophthalmic branch of the internal carotid artery (Fig. 1-19). The deepest structures in this region of the cheek are the buccinator and levator anguli oris muscles. Unlike the other muscles of facial expression, the buccinator is a relatively fleshy muscle. It lies within a drop-down plane covered by a significant amount of fatty tissue, often referred to as the buccal fat pad (Fig. 1-25). The buccinator is pierced by the parotid duct as well as blood vessels and buccal branches of the maxillary nerve en route to supply sensory innervation to the buccal mucosa.4,9,22 The buccal fat pad itself lies technically in the medial cheek. This fatty mass is well defined and contained by a thin layer of fascia, and on its surface the facial nerve branches can be visualized crossing over the fat pad still deep to the SMAS (Fig. 1-6). Superiorly, the infraorbital nerve branches out as a leash of nerves to supply sensory innervation to the medial cheek. The supraorbital foramen is easily palpated on most individuals.
The masseter–parotid region offers a very important anatomical landmark—the deeply set masseter muscle. A muscle of mastication supplied by the trigeminal nerve, the masseter can be easily visualized and palpated when the jaw is clenched. Its strong attachments extend between the zygomatic arch and the ramus of the mandible, and its anterior musculotendinous border provides an important landmark for key facial structures. The posterior half of the masseter is covered by the parotid gland. Contained
within its own fascia, the parotid gland, wedged along the preauricular mandibular region, is separated from the masseteric fascia which is a continuation of the superficial layer of deep cervical fascia. The lower anterior portion of the masseter may be overlapped by the fibers of the platysma in most individuals.
When visualized on unembalmed cadaveric specimens, the parotid gland displays a yellowish color, very similar to the living patient. It may sometimes be confused with subcutaneous fat as it is relatively close to the skin itself (Fig. 1-23). Unlike the subcutaneous tissue, however, the parotid gland is contained within a shiny, tight fascial sheath, the parotid fascia, which may help in differentiating it from fat. On the anterior border of the gland, the parotid duct can be located as it travels horizontally and then downward into the buccal fat. It consistently crosses over the masseter muscle before turning sharply toward the buccinator to pierce it and enter the oral cavity opposite the upper second molar. From its surface anatomy, the parotid duct may be located in the region of intersection between the tragolabial line,22 and the anterior edge of the masseter muscle and, additionally, along the zygomatic arch about 2 cm below it. The parotid duct is a prominent structure and provides a reliable anatomical landmark. As the parotid duct lies deep to the SMAS, it is crossed by fibers of the zygomatic branch of the facial nerve and also flanked by the upper and lower buccal branches of the facial nerve (Figs. 1-5, 1-6, and 1-23).
The transverse facial artery, arising from the external carotid artery, passes parallel to the parotid duct between it and the zygomatic arch. It also crosses over the anterior margin of the masseter muscle. The superficial temporal artery exits the parotid fascia below the zygomatic arch just anterior to the tragus (Fig. 1-27).4,9,22 It passes posterior and deep to the parotid gland as one of the terminal branches of the external carotid artery. The facial artery and vein (posterior to the artery) also travel beneath the SMAS as they cross over the mandible. The facial artery and vein can be located just anterior to the masseter muscle. The facial artery, which travels in a tortuous ascending course, is often more prominently tortuous in older individuals. The mandibular branch of the facial nerve crosses over the facial artery about 5 to 10 mm above the point at which the facial artery crosses the mandible.
The mandibular region extends from the anterior margin of the masseter muscle to the chin. Three predominant muscles are encountered after reflecting the skin in the region. The platysma lies within the superficial fascia and inserts into the skin of the lower lip, blending in with the fibers of the orbicularis oris muscle. The depressor anguli oris, which originates on the mandible and inserts onto the angle of the mouth, also sends fibers that blend in with those of the platysma and orbicularis oris.
Both the facial artery and the marginal branch of the facial nerve lie deep to the fibers of the platysma. In most individuals, the marginal branch of the facial nerve maintains a course above the mandibular rim, crossing the facial artery to supply the depressors of the lips and the mouth. While there are usually two branches, the mandibular branch of the facial nerve can exist as a single nerve or have as many as four branches (Fig. 1-26).
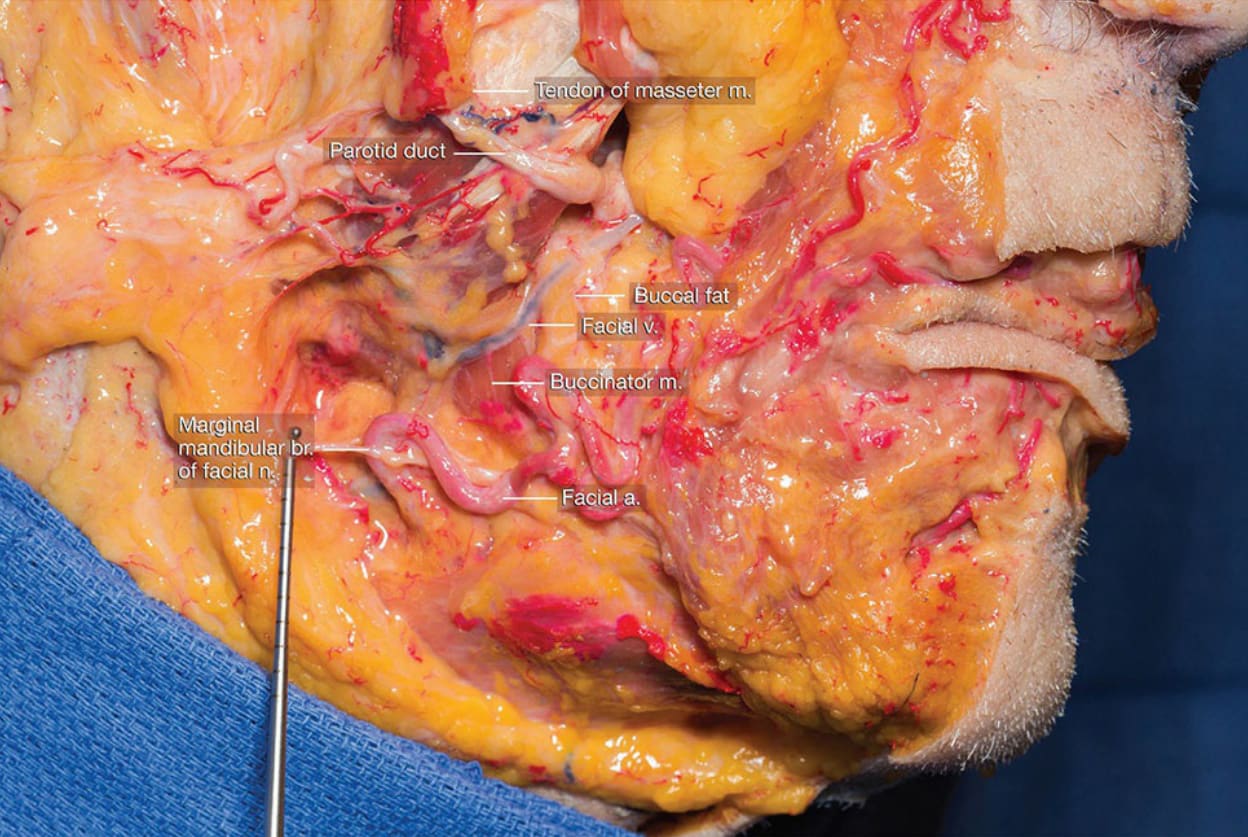
Figure 1-5. Deep dissection of facial nerve with reflected upper portion of parotid gland.
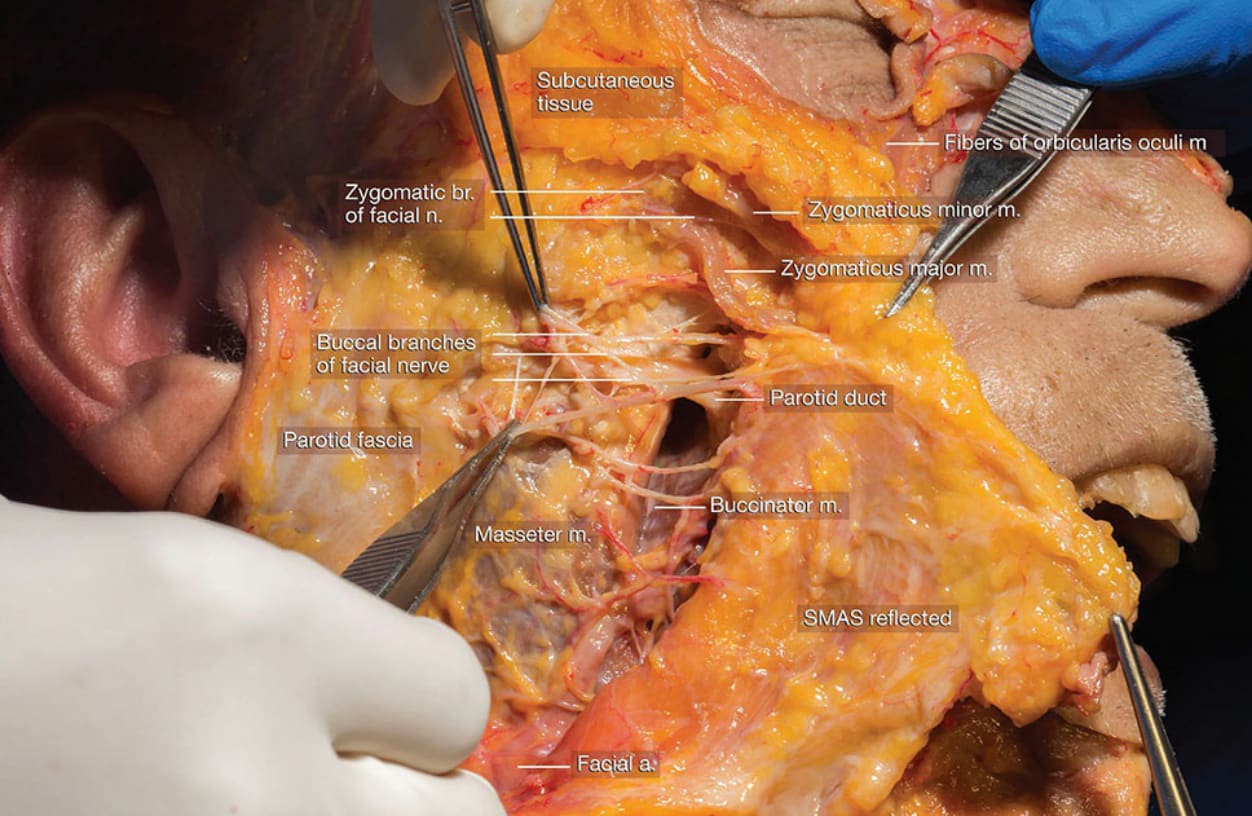
Figure 1-6. Dissection of facial nerve deep to SMAS.

Figure 1-19. Dissection demonstrating ascent of the facial and angular artery within the nasolabial region.
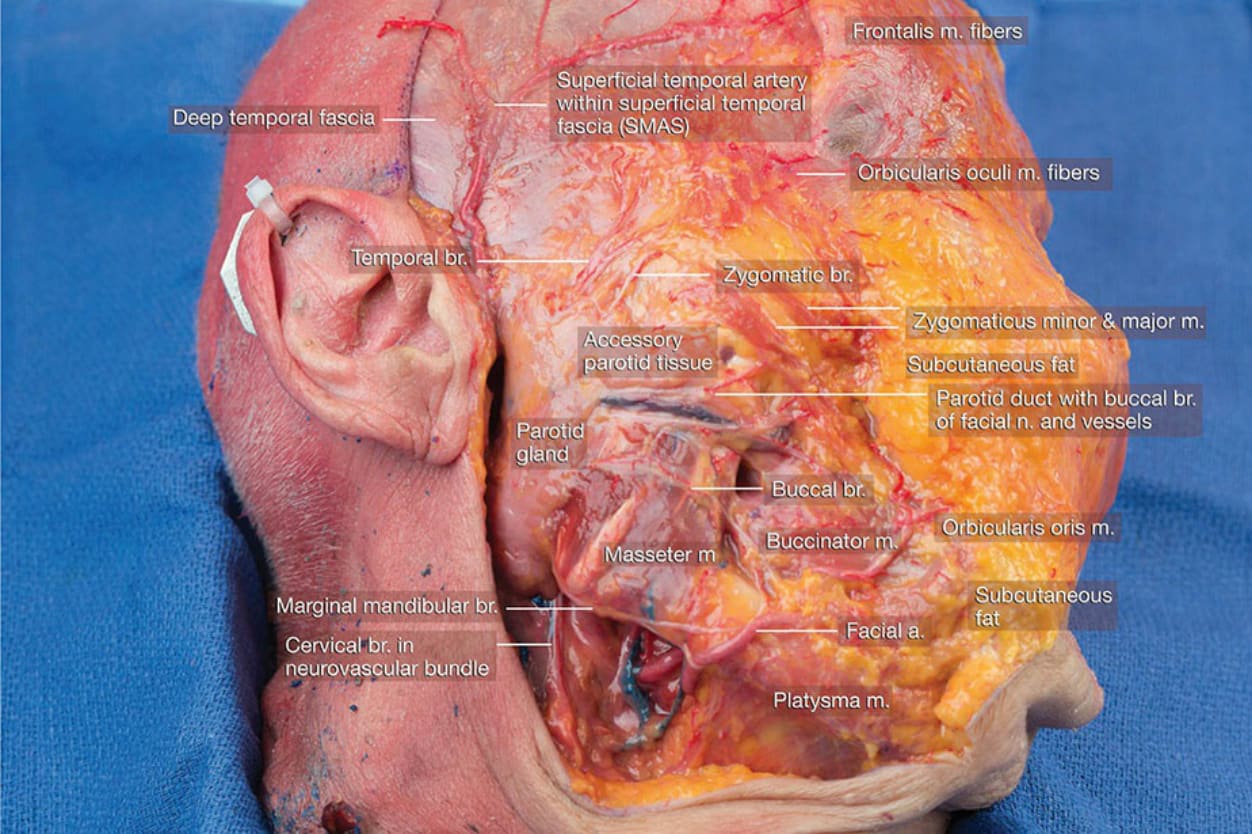
Figure 1-23. Dissection of the lateral face with skin and subcutaneous layers reflected medially.
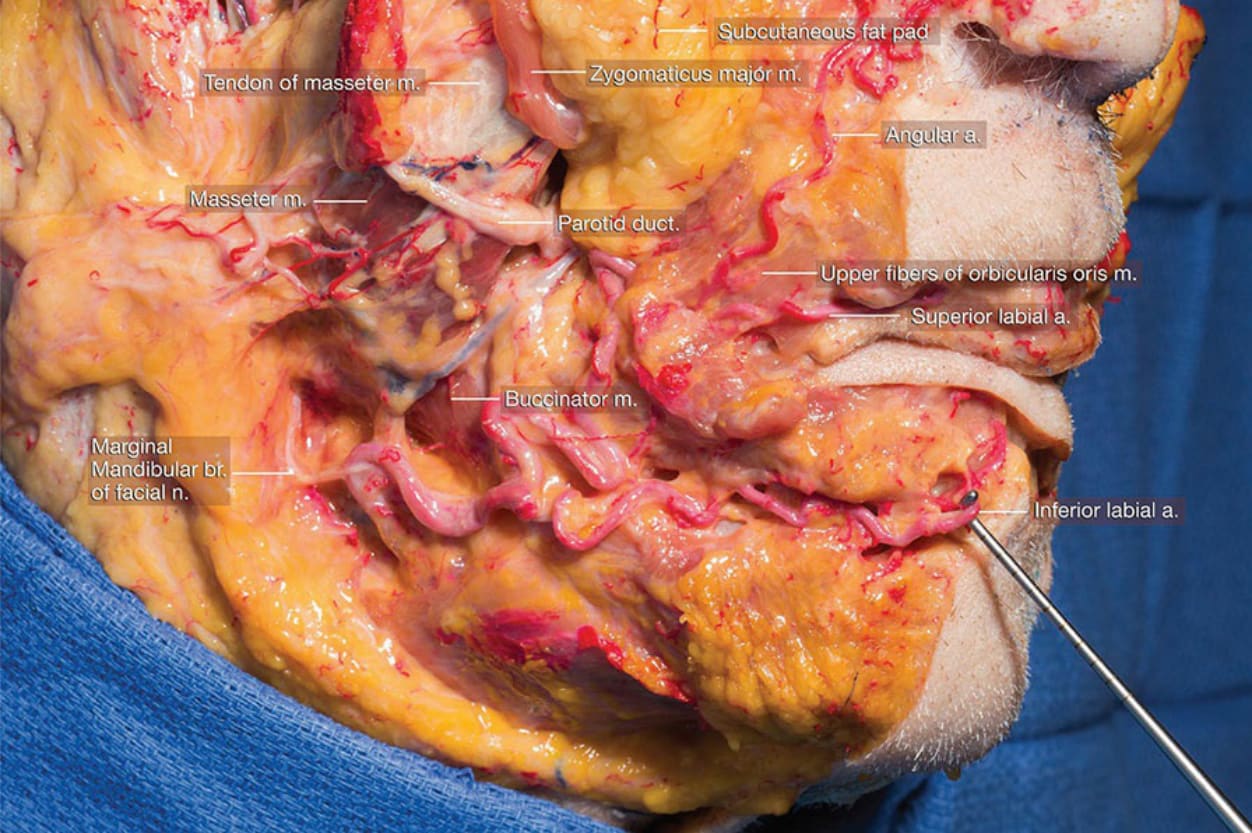
Figure 1-25. Lateral view of dissection of regional anatomy around the mid cheek and mandibular region.

Figure 1-26. Dissection highlighting the marginal mandibular branch of the facial nerve and its relationship to the facial artery.
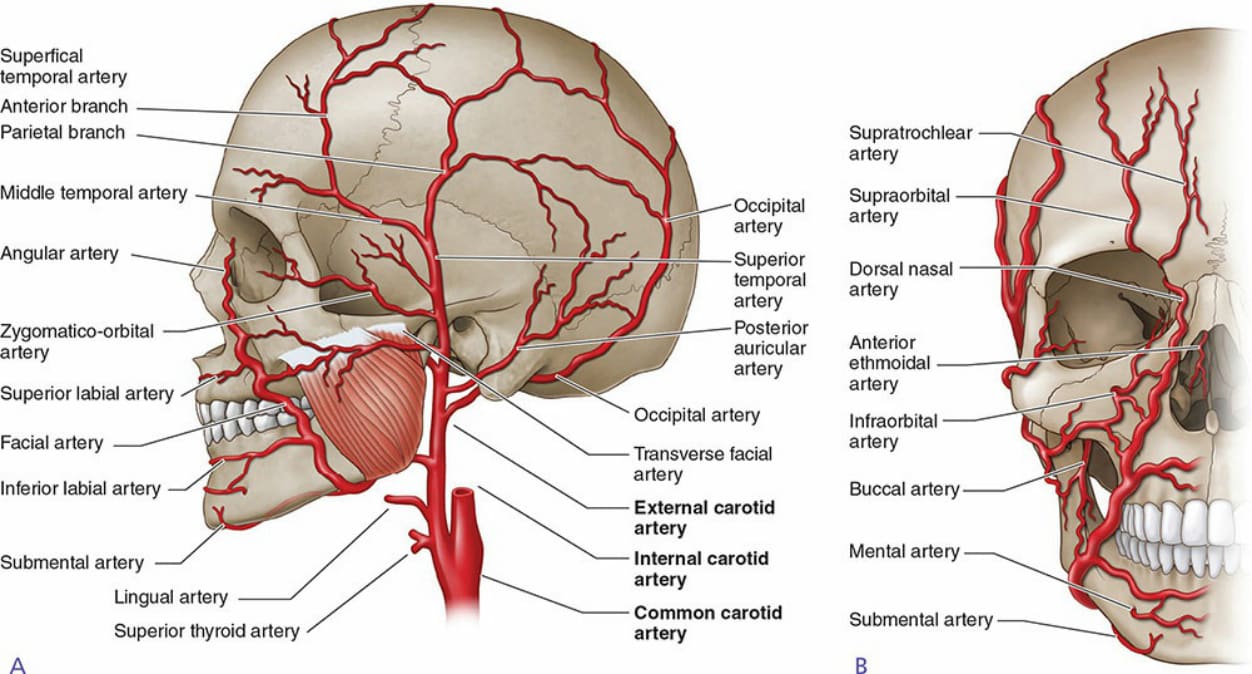
Figure 1-27. Diagram illustrating the arterial pattern and supply to the face.