Nose
Nose
The nose is divided into root, dorsum, lateral walls, tip, alae, and columella.
Most of the alae are composed of skin and fibrofatty tissue.
Blood supply is mainly from angular artery externally and the sphenopalatine
artery internally, with smaller contributions from the superior labial and ophthalmic arteries.
Sensory innervation is derived from infraorbital branch of the maxillary nerve and
infratrochlear and external nasal branches of the anterior ethmoidal nerve (ophthalmic nerve).
The challenge with conducting surgery on the nose is twofold. On the one hand, the nose presents with complex anatomy consisting of skin, cartilage, and nasal mucosa within a rather small anatomical boundary. Secondly, the mid-face location of the nose places a premium on cosmetic outcome, which reinforces the importance of thoroughly understanding the anatomy that will facilitate effective surgical repair and outcome. In its simple description, the nose may be divided into the root, dorsum (bridge), lateral side walls, and the lobule (Fig. 1-17). The lobule is further divided into the nasal tip, the infra-tip, and the alae. When viewed from below, the infra-tip lobule presents a soft triangular area anteriorly, a columella that extends inferiorly and separates two nostrils bound by the nostril sills, and laterally the alar base and rim. Together, the bony pyramid, septum, alar cartilages, and the cartilaginous vault form the main structural support of the nose.
The nasal bones articulate along the midline and with the frontal processes of the maxillae laterally. Superiorly, the nasal bones articulate with the nasal processes of the frontal bone and inferiorly with the perpendicular plate of the ethmoid bone. Nasal bones are thickest superiorly but thin out inferiorly where they may be easily damaged. There is an overlap between these lower and upper borders of the lateral cartilages. Skin over the bony pyramid is loose, fairly mobile, and can be easily undermined.22,23
The lateral cartilages are a continuation of the nasal bones, being overlapped superiorly by these bones and inferiorly by the upper border of the lateral crura of the alar cartilages. Ligamentous tissue connects both these overhangs.
The nasal septum consists of bone, cartilage, and soft tissue which include all of its articulating craniofacial bony structures. A septal or quadrangular cartilage anchors to the perpendicular plate of the ethmoid bone and maintains structural integrity of the bony septum. The membranous septum, a soft tissue composite, consists of two layers of vestibular skin separated by loose connective tissue. Depressor septi muscle traverses the membranous septum and attaches to the inferior border of the septal cartilage.4,22
The lobule is the most mobile portion of the nose due to the lack of any fixed cartilaginous joints. The support of the lobule comes from the paired alar cartilages suspended by soft tissue ligaments. The soft tissue portion of the ala does not contain cartilage but rather is structurally maintained by a thickened dermis with no underlying subcutaneous fat, making detecting an ideal dissection plane challenging in this area.
The key muscles around the nose include procerus, levator labii superioris alaeque nasi, nasalis, and depressor septi muscles. Procerus extends from the frontalis muscle across the root of the nose and blends in with the transversely positioned nasalis muscle. It is important to remember that the plane deep to nasalis is continuous with the subgaleal plane, which maintains a bloodless field of dissection. The levator labii superioris alaeque nasi arises from the maxilla and sends fibers to the medial upper lip and the lateral ala. The most medial portion of these muscle fibers is referred to as the depressor septi, which pulls down on the septum and keeps the airways patent (Fig. 1- 18).
The nose receives a rich blood supply which is a surgical advantage and allows for versatility in flap design and orientation. While blood supply is mainly from the angular artery externally and the sphenopalatine artery internally, with smaller contributions from the superior labial and ophthalmic arteries, the largest vascular contribution is derived from the external carotid system. The superior and inferior labial arteries are branches off the facial artery and they continue along the lateral aspects within the nasolabial grooves as the ascending angular artery en route to the medial canthal anastomotic site. The angular artery gives off many small branches to the sidewalls, ala, and dorsum, and form free and contralateral anastomoses terminating through a connection with the dorsal nasal artery (Fig. 1-19). This point of anastomosis is highly predictable, and its consistent presentation makes it a very viable pedicle for flap construction. The glabella and mid-portion of the forehead is supplied by the supratrochlear artery, a branch of the ophthalmic artery that is also a reliable vascular
pedicle in nasal reconstruction of the dorsum and tip of the nose (Fig. 1-20). Deep to the nasal bone, the external nasal artery emerges onto the dorsum of the nose (Fig. 1-21). It is usually accompanied by the external branch of the anterior ethmoidal nerve which supplies sensory innervation to the dorsum and tip of the nose. The infraorbital artery also contributes to vascular anastomosis around this area. Venous drainage follows the pattern of arterial supply and does not display any anatomy of significance.
Sensory innervation to the nose is achieved through branches of the ophthalmic and maxillary divisions of the trigeminal nerve. Ophthalmic division supplies the area along the midline of the nose, whereas the maxillary division via the infraorbital nerve (Fig.
1-20) innervates the alae, lower lateral walls, and columella. The root and upper nasal bridge along with the upper lateral walls is supplied by the infratrochlear nerve that approaches the nose in a medial direction from above the medial canthal tendon.
Ear
The external ear is divided into the auricle (pinna), the external auditory meatus
and canal, and the external surface of the deeper set tympanic membrane.
Blood supply to the ear is derived from superior and inferior auricular branches of
the superficial temporal artery and the deep auricular branch of the maxillary artery.
The external ear receives a rich sensory innervation from overlapping cranial and
cervical nerves.
The auriculotemporal nerve travels posterior to the superficial temporal vessels
and supplies the anterior portion of the auricle and anterior helix.
The auriculotemporal nerve lies posterior to the superficial temporal artery and
vein, and exits the superior parotid fascia as it traverses the parotid gland.
The mastoid area is supplied by C2, C3 ventral rami derived via the lesser
occipital nerve. Concha is supplied by variable overlapping innervation from cranial nerves VII, IX, and X, which also supply the posterior aspect of the external meatus and tympanic membrane and posterior auricular sulcus.
For the dermatologic surgeon, understanding the architecture of the ear is essential to repairing both large and smaller defects. When undermining, performing a primary closure, or during mobilization, knowledge of the variation in skin thickness, elasticity, relationship to the underlying cartilage, and pattern of perfusion helps in producing the most effective repair.
The external ear is divided into the auricle (pinna), the external auditory meatus and canal, and the external surface of the deeper set tympanic membrane.22 The auricle consists of a complex cartilaginous framework that is thrown into folds and grooves. The cartilage is covered by tightly bound skin with very little subcutaneous tissue, often with no subdermal fat at all. While the skin is tight anteriorly, posteriorly it offers a little more flexibility. The most inferior portion of the auricle, the lobule, has no cartilaginous base and consists of subcutaneous fat and skin. There are two distinct curves that extend superior to the lobule: (1) the outer helix—an anteriorly curved fold that continues posterosuperiorly from the lobule toward the upper limit of the tragus where it blends in with the crus of the helix; and (2) the antihelix, separated from the helix by a groove known as the scaphoid fossa. The tragus, an anterior extension of the auricular cartilage, is separated from the antitragus by the intertragal space. A deep concave groove referred to as the concha leads to the external auditory meatus. The concha is further subdivided into a more superior impression, the cymba, and an inferior, larger impression, the cavum (Fig. 1-22).4,9,22
While variations exist, in its standard anatomical position the ear is situated laterally, lies somewhat between the eyebrows and the base of the nose with the helix protruding beyond the antihelix. Ligamentous fibers connect the auricle to the skull and contain rudimentary intrinsic muscles. Extrinsic muscles are of little clinical significance, but it is helpful to note that these muscles of facial expression—the anterior, posterior, and superior auricular muscles—are contained within the SMAS and innervated by branches of the facial nerve.
The length of the external auditory meatus and canal measures 2.5 to 3.5 cm. The canal itself has both bony and cartilaginous parts.22 Laterally, the cartilaginous component is continuous with the auricular cartilage, while medially, it is attached to the bony meatus. The cartilaginous portion is mostly present in the inferior aspect of the canal. Superiorly, the canal is bound by the squamous temporal bone. The true bony portion of the canal tunnels between the squamous and tympanic parts of the temporal bone. Around the lateral portion of the external meatus the skin is thicker, with sebaceous, cerumeniferous glands and hair. The bony portion contains very thin layer of epithelium and is devoid of hair and glands. Of particular clinical interest are the fissures within the cartilaginous portion of the canal. These randomly arranged fissures, known as fissures of Santorini, offer potential avenues for developing skin cancers to spread into surrounding tissue.
The rich blood supply to the ear is derived from superior and inferior auricular branches of the superficial temporal artery and the deep auricular branch of the maxillary artery. Additionally, the posterior auricular artery, a branch of the external carotid artery, supplies the posterior aspect of the ear. Arterial branches are arranged as a single layer of vessels within the skin as a consequence of the sparsity of subcutaneous fat. The venous pattern corresponds with the arterial supply, and drainage is via the superficial temporal and retromandibular veins.
The external ear receives rich sensory innervation from overlapping cranial and cervical nerves. The mandibular division of the trigeminal nerve gives off the auriculotemporal nerve, which travels posterior to the superficial temporal vessels and supplies the anterior portion of the auricle and anterior helix. Additionally, the auriculotemporal nerve supplies the anterior and superior walls of the auditory canal as well as a portion of the external surface of the tympanic membrane (Fig. 1-13). Injury to the auriculotemporal nerve may be limited by recalling that it lies posterior to the superficial temporal artery and vein and that inferiorly it exits the superior parotid fascia as it traverses the parotid gland. The great auricular nerve (C2, C3 ventral rami) supplies most of the medial surface of the auricle as well as the posterior portion of the lateral surface of the auricle. This will include most of the helix and antihelix. The mastoid area is also supplied by C2, C3 ventral rami but its innervation is derived via the lesser occipital nerve. The concha is variably innervated by cranial nerve VII, and the meatus is innervated by cranial nerves IX and X.4,9,22 These cranial nerves also supply the posterior aspect of the external meatus and tympanic membrane and posterior auricular sulcus.
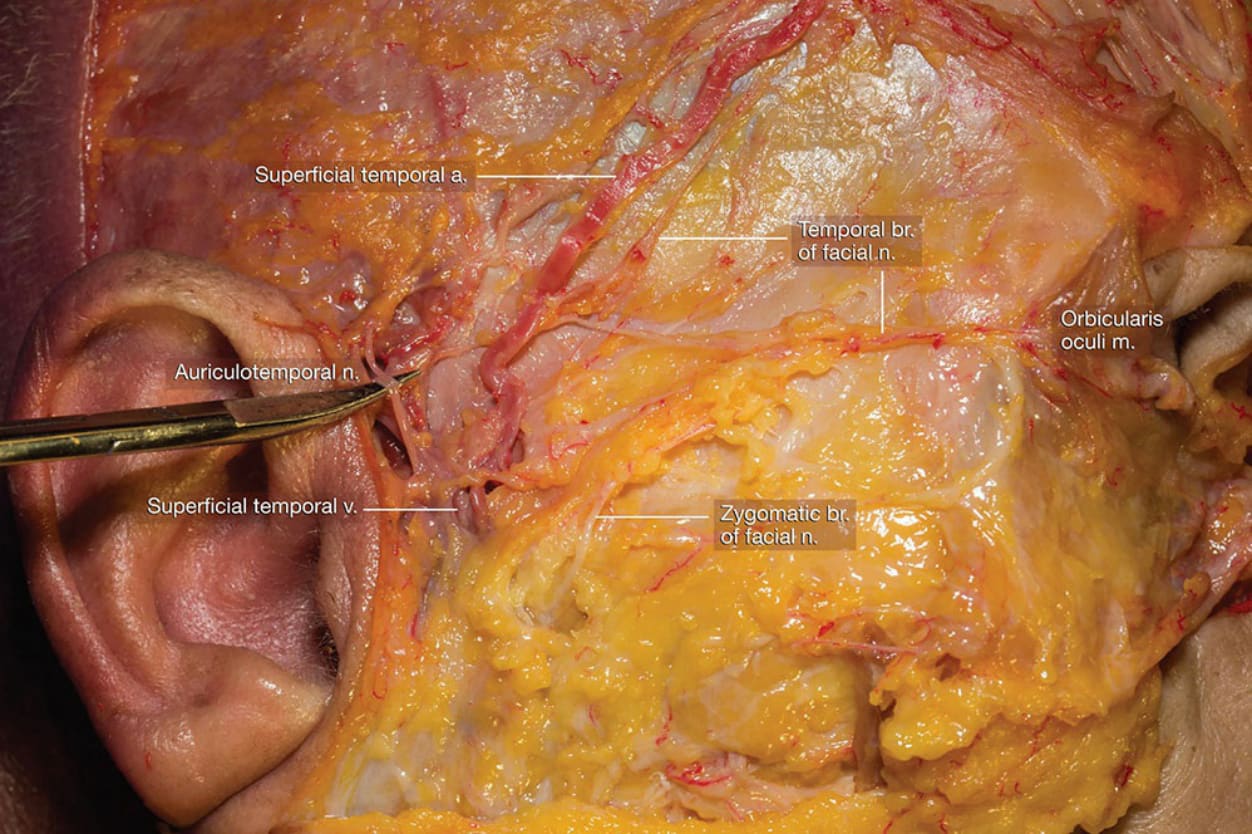
Figure 1-13. Dissection of temporal region highlighting the auriculotemporal nerve.
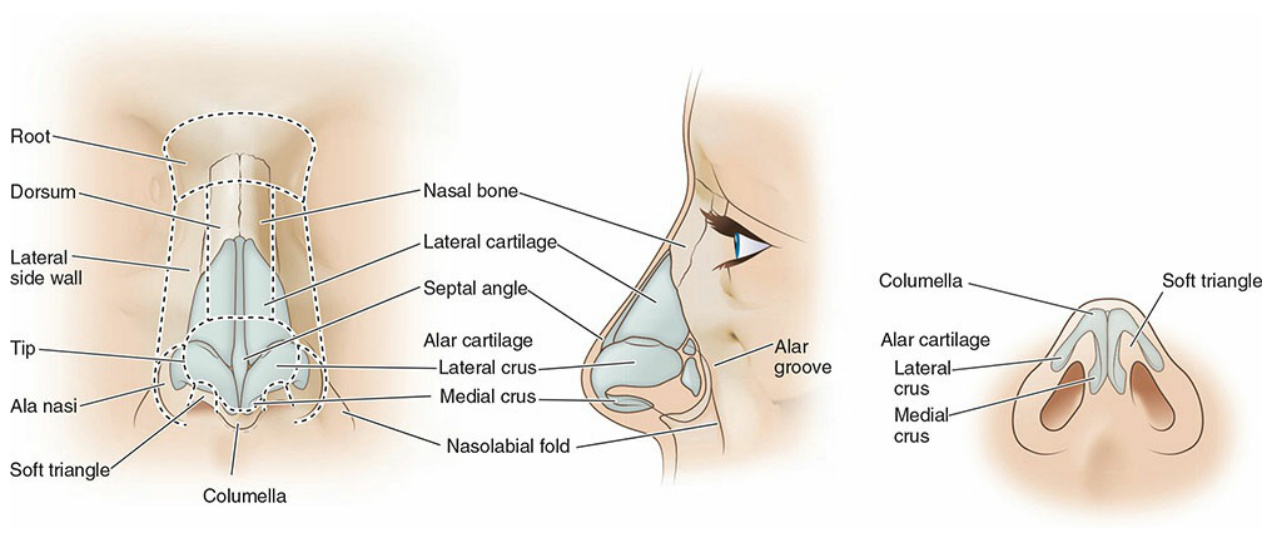
Figure 1-17. Diagram illustrating basic anatomy of the nose.
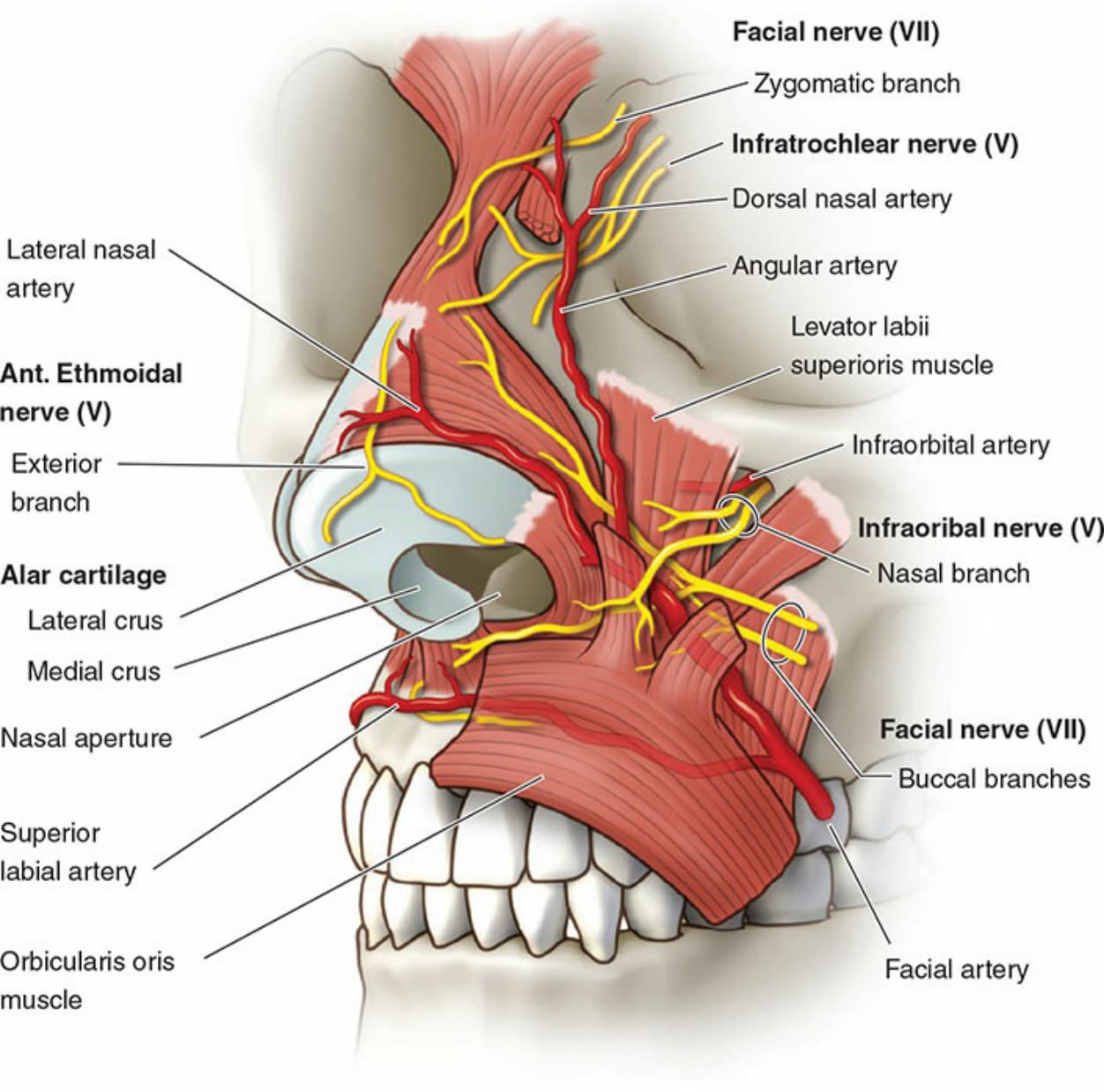
Figure 1-18. Diagram illustrating deeper anatomy around the nose.

Figure 1-19. Dissection demonstrating ascent of the facial and angular artery within the nasolabial region.

Figure 1-20. Dissection of the anterior left cheek highlighting the infraorbital nerve.
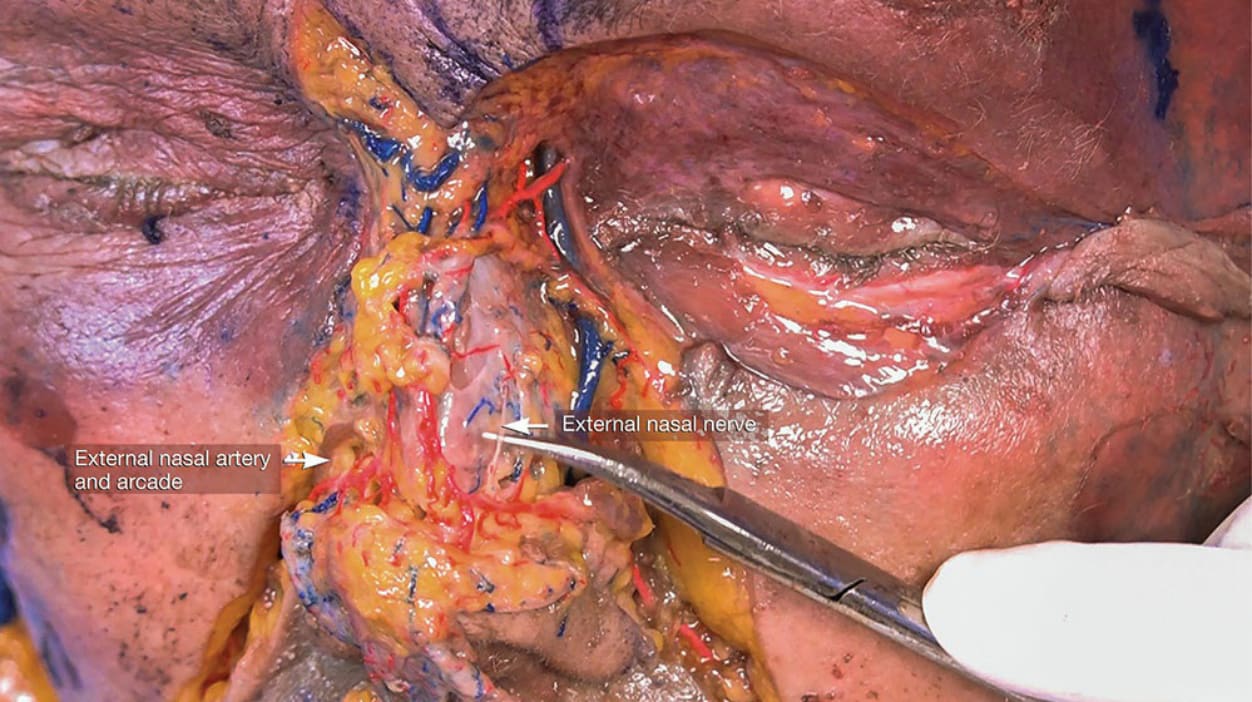
Figure 1-21. Superficial dissection of anterior nose demonstrating the external nasal nerve and vessels.
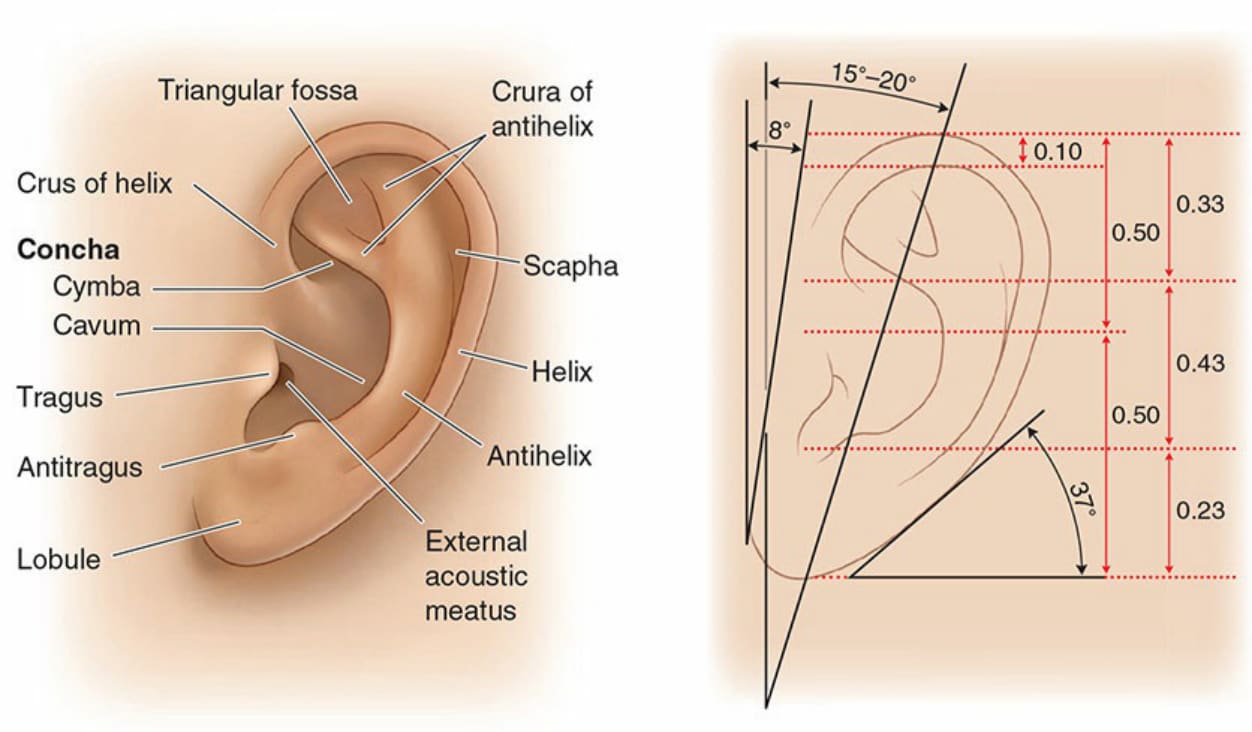
Figure 1-22. Diagram illustrating basic anatomy of the external ear.