Background
Background
Laser treatment of erythema and telangiectasias is based on the theory of selective photothermolysis: the chosen wavelength of light should correspond to the absorption peak of the target structure and the pulse duration should be equal to or less than the thermal relaxation time of the target structure. This principle dictates that selective destruction of the target takes place with minimal damage to surrounding structures.
For erythema and telangiectasias the target structure is usually oxyhemoglobin within the vessels, as this comprises the majority of total hemoglobin. To understand the best wavelengths to treat superficial red vessels, one must know that oxyhemoglobin’s primary absorption peaks are in the blue–yellow–green portion of the visible light range (418, 545, and 577 nanometers [nm]); the lowest wavelength peak of 418 nm is strongly absorbed by melanin, however, and therefore should not be utilized for vascular lasers (Fig. 77-5). Even light with wavelengths at the peak of 542 nm will have too much absorption by melanin and therefore fail to be photoselective for hemoglobin, resulting in probable epidermal damage, unless cooling is used to protect the epidermis.
The fourth broadband hemoglobin absorption peak from 700 to 1,100 nm becomes more important when targeting deeply seated vessels. In general, longer wavelengths penetrate more deeply into the skin with less scattering of photons and greater penetration to a deeper target. Not only do longer wavelengths penetrate more deeply, but they also heat the target more uniformly.
The pulse duration is determined by the thermal relaxation time; larger diameter telangiectasias require longer pulse duration to allow sufficient time for diffusion of heat evenly throughout the cylindrical vessel (Table 77-1). Shorter pulse durations may be needed for smaller vessels, but can result in excessive heat and vessel rupture, and thus increased risk for purpura. In general, longer pulse durations of at least 6 ms (and up to 40 ms) are used for telangiectasias to decrease risk for purpura. Larger spot sizes result in less scattering and deeper penetration.
While delivering a sufficient quantity of energy to thermocoagulate the target vessel, the overlying epidermis should be unharmed. This requires minimization of absorption by melanin and some mode of protective epidermal cooling. A number of different laser and IPL systems have been developed with this goal in mind. Cooling may be applied by direct contact, cold gel, cold air blowing, or spray cryogen. Cooling may also be applied before, after, or continuously during the laser pulse. In patients with higher Fitzpatrick skin types, there is a risk of depigmentation, hypopigmentation, and postinflammatory hyperpigmentation with cryogen spray if excessive. Contact cooling can be achieved via sapphire crystal, quartz, or copper. Sapphire crystal maintains cold temperatures better than the others. With contact cooling it is important to maintain proper contact with the skin, otherwise the risk of epidermal damage increases. Fluence needs to be adjusted on the basis of baseline vessel temperature; the colder the vessel from prechilling, the higher the fluence required.
Table 77-2 lists the most commonly used lasers to treat erythema and telangiectasias. Pulsed-dye lasers (PDLs), potassium titanyl phosphate (KTP) laser, alexandrite laser, Nd:YAG, and infrared diode lasers as well as IPL devices are typically used. There are several caveats when considering a laser of choice. KTP laser is actually a laser beam generated by a neodymium-doped yttrium aluminum garnet (Nd:YAG) laser, which is then directed through a KTP crystal to produce a coherent light in the visible green portion of the spectrum. The 532-nm wavelength is one of several hemoglobin absorption peaks. Absorption of melanin is significant, and thus KTP lasers are not recommended for those with Fitzpatrick skin types above III or patients who are significantly tanned.
PDL produces light in the yellow spectrum and has less absorption by melanin. The alexandrite laser is significantly absorbed by epidermal melanin, and so is best for patients with lower Fitzpatrick skin types. As the 1,064-nm wavelength’s interaction with melanin is much less than that of other laser wavelengths utilized for hemoglobin, its use allows treatment of skin types up to Fitzpatrick V, something not possible with other wavelengths. Because the Nd:YAG laser heats water within the epidermis and dermis, there is a higher risk of overheating the skin with possible resultant epidermal/dermal injury, and eventual hypopigmentation, depigmentation, atrophy, and scarring. Therefore, the smallest spot size and lowest energy should be adopted when using this wavelength. In addition, clinical endpoints, such as blurring of vessels, can be less clearly visible, so there is a risk of overtreatment and thus increased risk of side effects. Lastly, diode lasers have varying wavelengths in the infrared region which pick up the fourth peak of hemoglobin, but are infrequently used to treat vascular lesions as there is a risk of epidermal damage. Historically they were used more often, but with the advent of lasers specific for hemoglobin their use has declined.
An IPL device consists of a noncoherent flash lamp that delivers controlled amounts of yellow, red, and infrared wavelengths to the skin. Theoretically, a device that produces a noncoherent light as a continuous spectrum longer than 550 nm should have multiple advantages over a single wavelength laser system. First, both oxygenated and deoxygenated hemoglobin should simultaneously absorb at these wavelengths. Second, larger blood vessels should be affected more than with a single wavelength. Third, thermal absorption by the exposed blood vessels should occur with less overlying epidermal absorption, as the longer wavelengths will penetrate deeper. Other advantages of this device are large spot sizes and the ability to control pulse duration and the length of the intervals between pulses, the latter of which is only possible with certain devices.
For IPL treatment of erythema and telangiectasias, shorter cutoff wavelength filters should be chosen; the value on the filter designates the shortest wavelength within it. Multiple filters may be employed to gain more selectivity, and notched filters are also now available with select systems. IPL devices satisfy the criteria for selective photothermolysis, permitting blood vessels to be selectively heated over the surrounding tissue. Pulses are typically separated to allow thermal relaxation time and cooling of the epidermis in between pulses. Modern IPL units include contact cooling and sapphire crystals to protect the skin.
The principles of laser treatment of erythema and telangiectasias are outlined in Table 77-3. Lasers should be analyzed in terms of the color of light they produce.
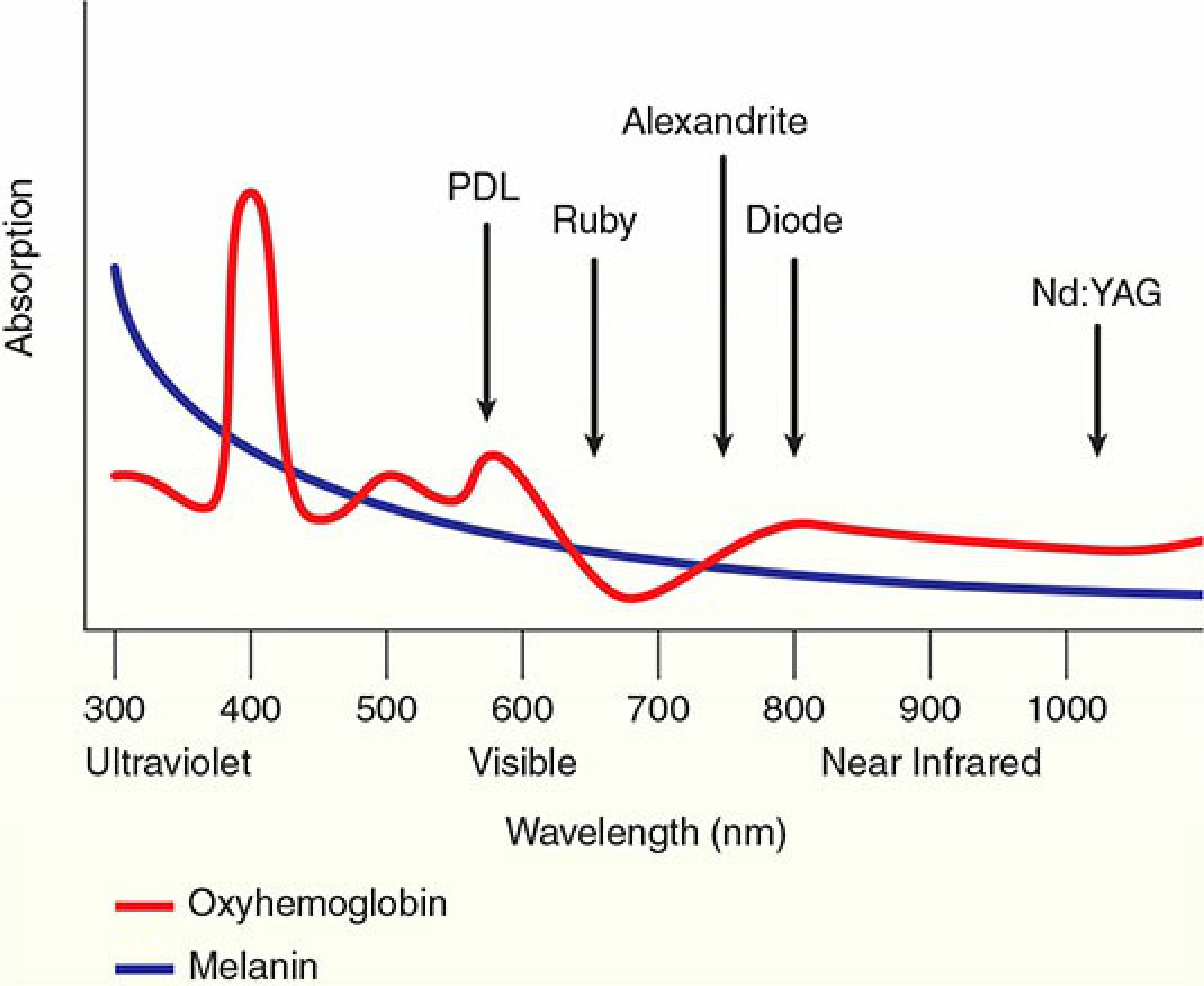
Figure 77-5. Absorption peaks for oxyhemoglobin and deoxyhemoglobin and relevant lasers.
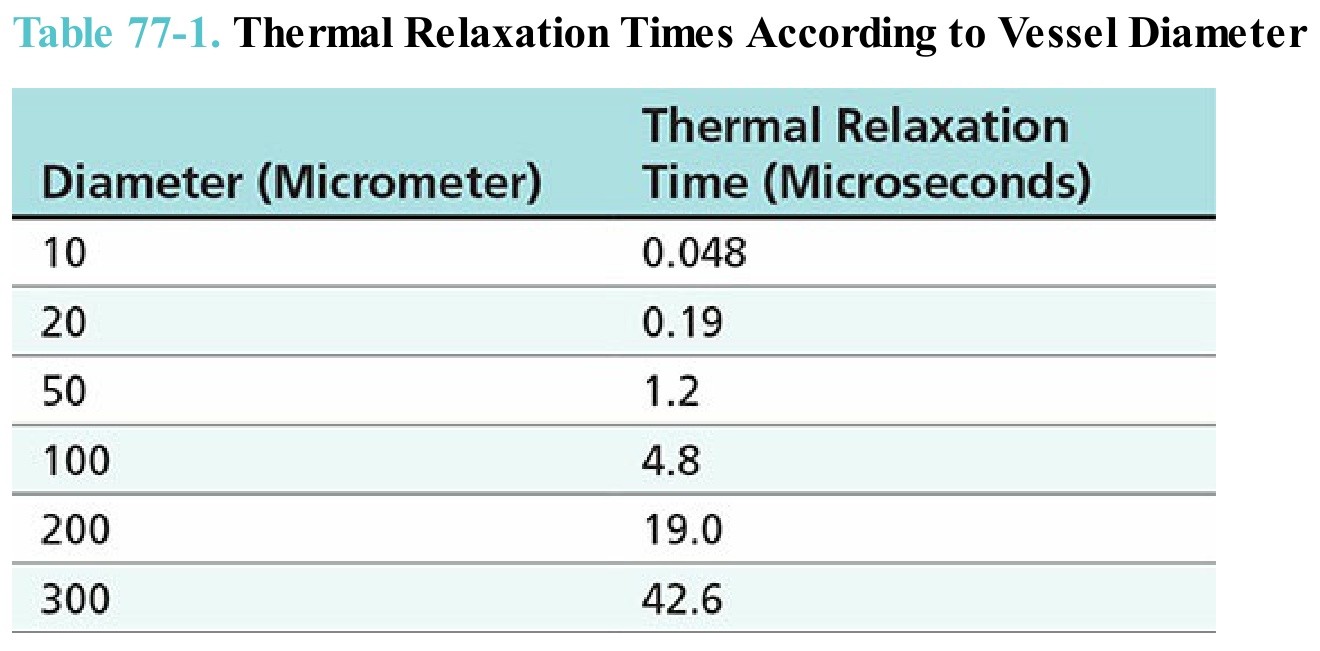
Table 77-1. Thermal Relaxation Times According to Vessel Diameter
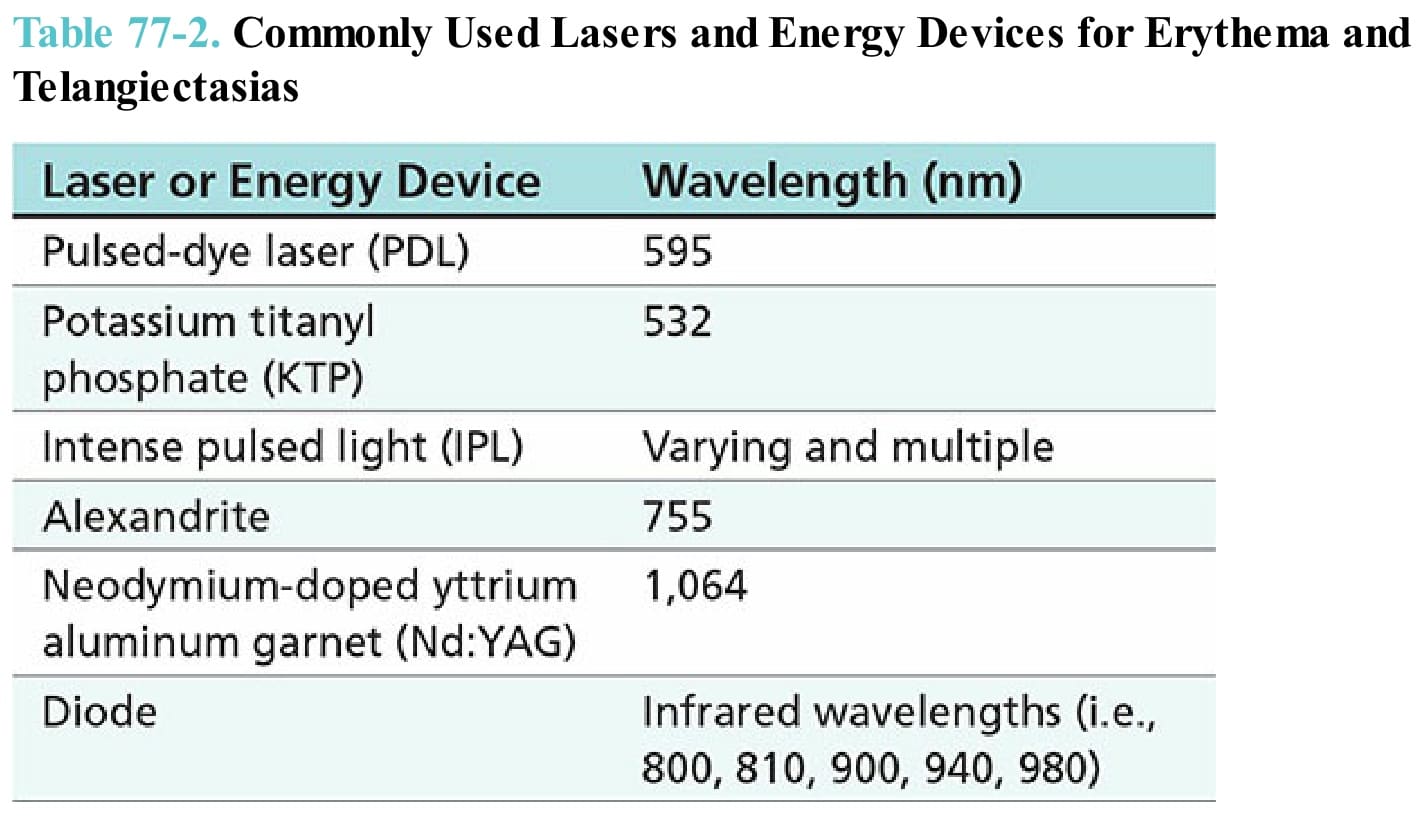
Table 77-2. Commonly Used Lasers and Energy Devices for Erythema and Telangiectasias
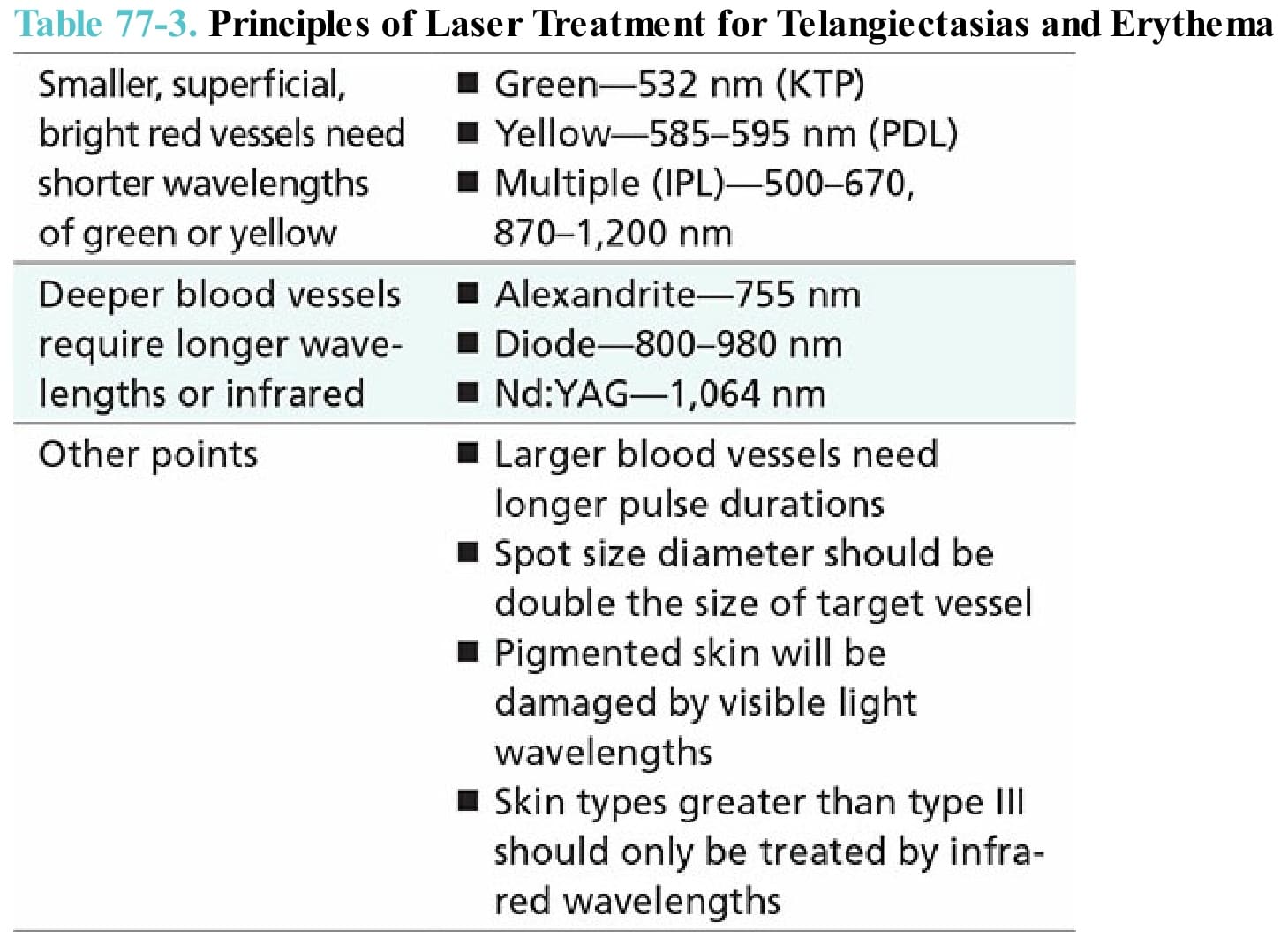
Table 77-3. Principles of Laser Treatment for Telangiectasias and Erythema