CRYOLIPOLYSIS
CRYOLIPOLYSIS
Cryolipolysis dates back to the 1970s, when Epstein and Oren observed a red indurated nodule followed by transient fat necrosis on the cheek of an infant who had been sucking on a popsicle. They termed this phenomenon “popsicle panniculitis,” which led to the discovery that adipose tissue is more susceptible to cold injury than surrounding tissue, a concept now referred to as “cold-induced panniculitis.”5 This idea was first exploited by Manstein et al. in 2007, who performed the initial studies exploring the selective destruction of fat.6 Using black Yucatan pigs, copper plates were applied at various
temperatures (–8, –7, –5, –3, –1, and 20°C) to a test site for 10 minutes. These areas were studied grossly and histologically at different time points, with the longest one being 3.5 months. They found that cooling induced a lobular panniculitis, and the amount of fat damage increased up to a month after exposure. This study was followed up by Zelickson et al. in 2009 using three pigs that underwent a single cryolipolysis treatment.7 They assessed the results histologically and by ultrasound, and found a 50% and 33% reduction, respectively, in the thickness of the superficial fat.
The mechanism of action for cryolipolysis and how it produces selective apoptosis in adipocytes remains unclear. One possible mechanism is that adipocyte death is caused by reperfusion injury which triggers free radicals, oxidative stress, and ensuing cell death. Under histologic analysis, there are no notable changes immediately after treatment. However, by day 3, an inflammatory process occurs and adipocytes become encircled by histiocytes, neutrophils, and lymphocytes. By 7 days, a lobular panniculitis is noticed. This process peaks at day 14, and between days 14 and 30, macrophages engulf the adipocytes and the inflammation decreases slowly over a 90-day period. Histologically, interlobular septae are thickened, and the fat volume is decreased by 2 to 3 months after treatment. Also, the epidermis, dermis, nerves, blood vessels, and muscles remain unharmed.2,4,8
In 2010, the first cryolipolysis device (CoolSculpting®, Zeltiq Aesthetics) was approved by the FDA for the reduction of abdominal and flank fat. Since then, its clinical indications have expanded to include fat reduction of the abdomen, flanks, upper arm, brassiere rolls, lumbar rolls, banana roll, thigh, and the submental area in individuals with a body mass index of 30 or less.9 During a typical 60-minute session, the area of fat is vacuum suctioned into a cup-shaped applicator which is attached to a central console via an umbilical cable. The console maintains a preset temperature, below 0°C, using sensors implanted in cooling plates on the sides of the applicator. The suction allows for maximum contact with the cooling plates and causes some vasoconstriction, allowing more rapid cooling of the skin.2,3
There have been numerous human clinical trials performed demonstrating the efficacy of cryolipolysis for selective fat reduction. In 2009, Dover et al. performed a trial using cryolipolysis on the flanks of 32 subjects. They assessed improvement using photography, physician assessment, and subject satisfaction.12 Ten subjects were further assessed by ultrasound of the treatment area. They found that all subjects had a reduction in the fat layer, with an average reduction of 22.4% seen by ultrasound. Another study by Kaminer et al. in 2009, treated 50 subjects with each serving as their own control.13 Each patient underwent cryolipolysis treatment of one flank and used photography and three blinded physicians to assess the subjects. The physicians could differentiate with an 82% accuracy rate between the treated and untreated side. The evidence from these two studies led to FDA approval for treatment of the flanks by
cryolipolysis. Further studies include those by Sasaki et al., who in 2014 treated six patients in a pilot study and then went on to treat 112 in the clinical treatment group.3 This demonstrated similar findings to previous studies, with an average fat reduction at 6 months of 21.5% by caliper measurements and 19.6% by ultrasound measurements (Fig. 68-1). They also found that massage in one patient after treatment led to more rapidly increased temperatures. In 2015, Ingargiola et al. published a review article evaluating 19 cryolipolysis clinical trials in humans.4 They found that average fat reduction ranged from 14.67% to 28.5%, as measured by caliper, and 10.3% to 25.5%, as measured by ultrasound.
Adverse events from cryolipolysis are generally mild, and include erythema, ecchymosis, swelling, sensitivity, and pain. Erythema is most common, occurs immediately, and can last for several hours after treatment (Fig. 68-2).11 Ecchymosis can be observed for days after treatment due to the vacuum suction used during the procedure, and is worse in patients taking anticoagulants.2,4 Transient numbness is another finding which was studied by Coleman et al. in 2009.14 He reported that six out of nine subjects experienced decreased sensation assessed by neurologic evaluation; however, this completely resolved after a mean of 3.6 weeks post-treatment. On biopsy,
there were no long-term changes observed in the nerve structure. Another very common complaint is pain. Most subjects experience a “shooting” or “cramping” pain within 1 week post–treatment. This is most likely due to the cold-induced panniculitis, and studies have found a correlation between increased pain and larger surface area treated. Most subjects reported that the pain was tolerable, could be controlled with oral analgesics, and resolved spontaneously over 1 to 4 weeks.2,8
In addition, there is a theoretical risk that lipid levels and liver function tests could possibly be increased due to the absorption of adipocytes by macrophages. However, multiple studies evaluating lipid levels and liver function tests (including aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, total bilirubin, and albumin) after treatment found no evidence of a significant increase in levels.15–18 One very rare side effect that has been observed is paradoxical adipocyte hyperplasia. This has been reported in 33 cases, and the exact mechanism of action is unknown. No spontaneous resolution has been reported, and the only treatment is liposuction or abdominoplasty.19 Contraindications to cryolipolysis include cold-induced conditions such as cold urticaria, cryoglobulinemia, and paroxysmal cold hemoglobinuria. It also should not be performed in areas with edema, dermatitis, varicose veins, or other cutaneous conditions.4 As far as patient satisfaction, Dierickx et al. performed a study in 2013 that reported 73% of 518 subjects were satisfied with their treatment and 82% would recommend the procedure to a friend.20 In that study, only 6 out 528 subjects were dissatisfied and 4 out of the 6 were satisfied after a second treatment was performed.
Overall, cryolipolysis has proved to be an effective means of selective noninvasive
fat reduction, with the best results seen in individuals close to their ideal body weight. Most people can expect to see an estimated 25% reduction in the fat layer with final results seen 3 months after treatment. Sometimes, a second treatment can be beneficial for targeting thicker areas, such as the abdomen.2
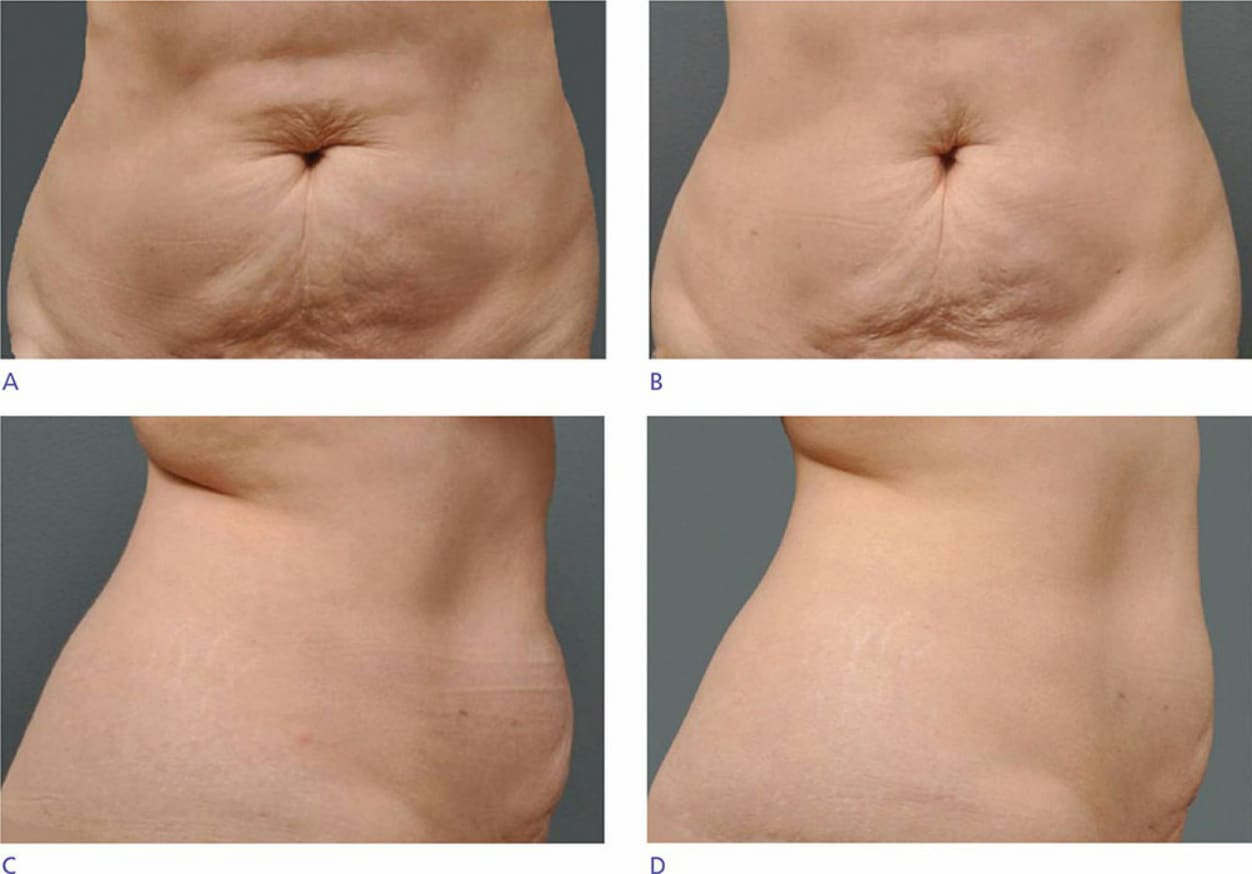
Figure 68-1. A 51-year-old female from the pilot study. (A,C) Subject’s pretreatment photographs. (B,D) Subject’s photographs 6 months after cryolipolysis treatment of her entire lower abdomen with a large applicator in a single session.

Figure 68-2. “The butter stick” erythema and swelling of the abdomen immediately post-treatment.