Surgical treatment of metastatic melanoma
Surgical treatment of metastatic melanoma
Distant metastatic melanoma (stage IV) indicates hematogenous spread and is associated with a 10-year survival of less than 10%.119 Surgery for metastatic disease is provided for palliation of life-threatening complications, or for curative intent. Common palliative indications include resection of brain metastases, resection of bowel metastases to relieve gastrointestinal obstruction, and treatment of regional disease that may be causing chronic pain or open wounds. Metastatic melanoma can present variably, ranging from rapid, diffusely disseminated disease in some patients to indolent oligometastases confined to a specific region in others. The mechanisms, both genetic and immunologic, underlying these different presentations are poorly understood.
However, in select patients with slowly progressing oligometastatic disease, there is potential that eradication of metastases will provide a survival benefit. Surgical resection offers long-term survival for a subset of patients with stage IV disease, with 5-year survival rates of 15% to 30%.120,121 The Malignant Melanoma Active Immunotherapy Trial (MMAIT) is commonly cited in support of metastasectomy. In this trial, patients with stage IV disease underwent complete surgical resection of metastases, followed by randomization for treatment with vaccine therapy. In both arms, the 5-year survival was at least 40%, markedly higher than any other phase III trial for stage IV disease, which has been attributed to surgical eradication of distant disease.122 Other trials provide evidence in favor of treating metastatic disease for select patients with the potential for eradication. In the Southwest Oncology Group trial (SWOG S9430), among patients who underwent complete resection, median survival was markedly increased to 21 months.123
For staging purposes, melanoma metastases are placed into three categories depending on the location: M1a, M1b, and M1c. M1a represents metastasis to soft tissue and distant nodes, M1b is metastasis to the lungs, and M1c represents visceral metastasis or any distant metastasis associated with an elevated lactate dehydrogenase (LDH) level. Skin and subcutaneous tissue metastases are associated with the best prognosis, followed by distant nodes, and surgical eradication of M1a disease may increase median survival up to 60 months based on retrospective analysis of MSLT-1 data.124 Skin, subcutaneous, and nodal metastases are generally detected earlier by the nature of their location, which may contribute to the improved survival of this category. Metastases to the lungs are frequently asymptomatic, and incidentally discovered on surveillance CT imaging. M1b disease is associated with a 1-year survival of 57%. Similarly, visceral metastases are often asymptomatic, though may manifest as gastrointestinal discomfort, obstruction or elevated liver serum markers. M1c disease is associated with the worst 1-year survival at 45%.119 Features of metastases based upon location are described in Table 46-7.
Appropriate patient selection for surgery remains an ongoing challenge for stage IV disease. Martinez et al. propose a set of qualification criteria: good functional status, life expectancy greater than 3 months, less than two separate visceral sites, and less than eight total metastases.126 Multiple other groups have put forth proposals with similar criteria. An important distinction is that complete metastasectomy provides superior survival outcomes compared to cytoreductive surgery.127 The decision to provide palliative surgery can be more challenging. Patients with pain, bleeding, or other symptoms such as gastrointestinal obstruction can often be effectively treated, though first requires careful consideration of multiple factors including projected survival, functional status, goals of care, and capacity to heal.
CONCLUSIONS
There have been great advances in the surgical management of melanoma over the last four decades, with marked improvement in survival for local and regional disease. Surgical techniques including biopsy, wide excision, sentinel node biopsy, lymphadenectomy, and isolated limb perfusion have been largely optimized from an operative standpoint, but the appropriate application of these procedures is an area of ongoing investigation. In the modern era, there still remain basic unanswered questions, including the appropriate selection of patients for node sampling with thin melanoma,
the value of CLND in clinically node-negative patients with positive sentinel nodes, and the appropriate selection of patients for resection of distant metastases. Going forward, advances in our understanding of melanoma biology will potentially allow for personalized surgical management of similarly staged lesions. Improved systemic therapies will likely reduce the need for morbid procedures including lymphadenectomy and metastasectomy. Finally, as more information about molecular, genetic and histopathological features of melanoma are applied to treatment and prognostication, collaboration between surgical and medical fields will be essential for effective application of this information to individualized care.
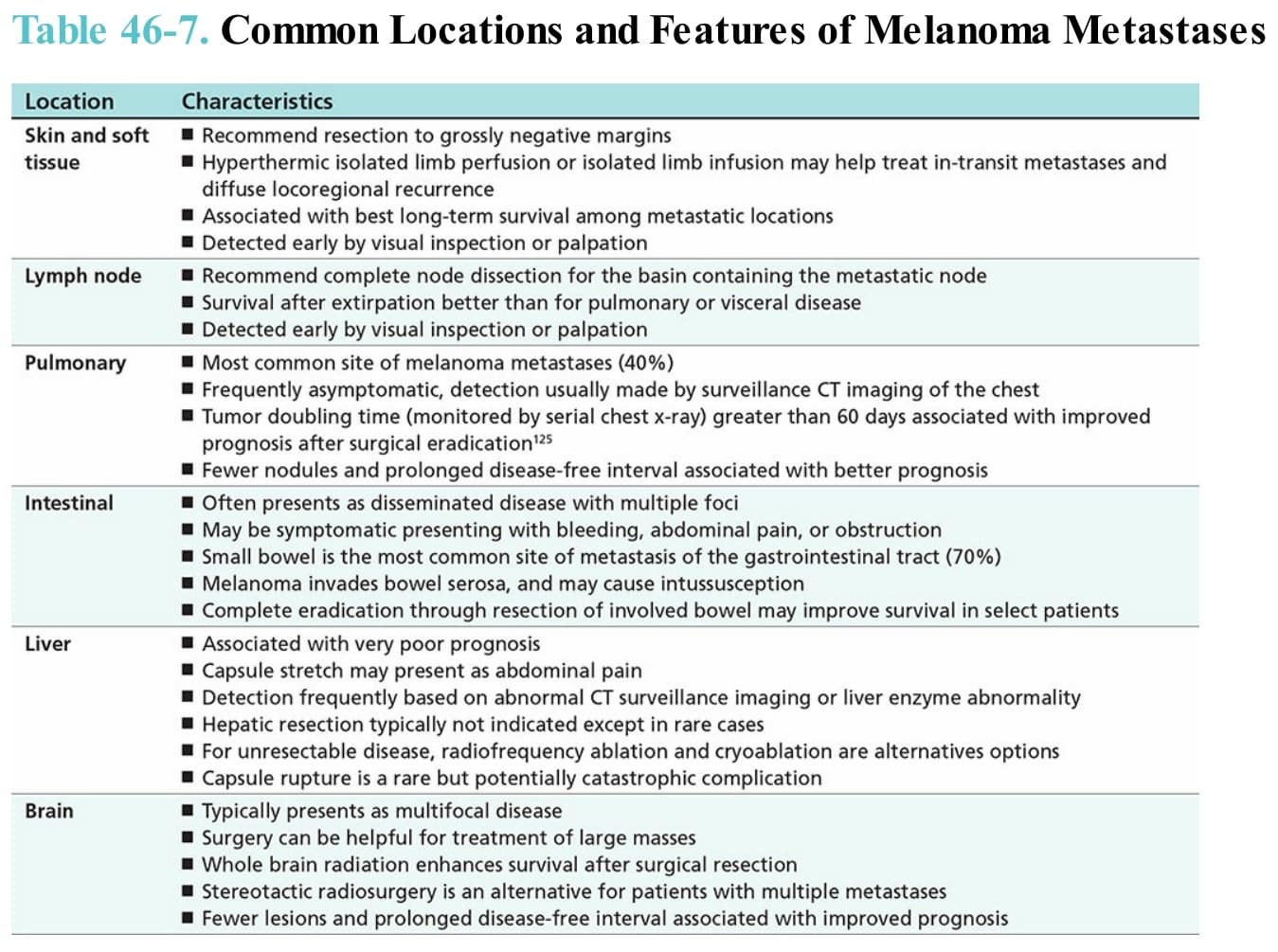
Table 46-7. Common Locations and Features of Melanoma Metastases