RESTRAINT
RESTRAINT
In addition to the forces involved in wound closure discussed above, a similar set of forces have been defined which serve to limit the primary motion of a flap. These factors serve as variants of restraint: negative vectors that work to counteract a flap’s primary movement.18
These vectors can be found in several different directions along a repair. The skin surrounding a raised flap exerts tension in the opposite direction of the new, desired movement of the tissue flap, creating horizontal restraint. The tissue underneath a flap, due to its connections to deeper structures in the skin, can exert deep restraint, a downward vector that may limit the desired movement of a flap (Fig. 20-5). Undermining around the flap pedicle, the wound base, and the surrounding skin involved in the repair may minimize the magnitude of this restraint. Extensive undermining, however, is not required, and may risk damage to critical structures and even impair blood flow. Most of the benefits from undermining are seen within the first 1 to 2 cm out from the wound edge.17
In flaps undergoing rotational movement, the pedicle, or attachment, creates a focus of pivotal restraint that can limit movement of the flap into the primary defect. The amount of pivotal restraint is also influenced by the elasticity of the skin and is magnified in thicker, less flexible skin and minimized in thinner, more elastic skin. This tethering can be seen in flaps such as rotation and transposition flaps (as well as many advancement flaps) that undergo pivotal movement, and must be taken into consideration when planning these repairs. Otherwise, the planned flap may not fill the primary defect, resulting in increased secondary movement, increased closure tension, and potentially distortion of neighboring free margins, anatomic boundaries, or flap-tip necrosis.
For rotation flaps, the leading edge of the flap can be extended to compensate for the rotational shortening caused by pivotal restraint. For transposition flap repairs, which involve two foci of pivotal restraint, the leading edge of the flap must be longer than the sides of the defect to avoid complications from pivotal restraint. Both of these modifications result in the necessity of removing a dog ear of redundant tissue during the repair because of the length discrepancy between sides; most importantly, however, this mitigates the risk of vascular compromise or anatomic distortion (Fig. 20-6).19
Redundant collections of skin or dog ears are often created during both flap repairs and fusiform closures due to the forced movement of tissue. Their presence creates obstructive restraint against primary flap movement as the extra tissue functions as a physical barrier, impeding the desired movement. The creation of standing cones is influenced by the presence of length discrepancies between wound edges, the required rotational angle of movement, skin elasticity, and the surface contour in the area of the repair. The pivot, or angle of rotation, and the size of the resulting standing cones are positively associated with one another; the larger the required angle of rotation, the larger the cutaneous deformity and thus obstructive restraint.15 Careful planning may decrease the significance of obstructive restraint; if standing cones of tissue were to develop, there are many surgical options which facilitate their removal and a proper closure, as detailed in Chapter 9 (Fig. 20-7).15,20,21
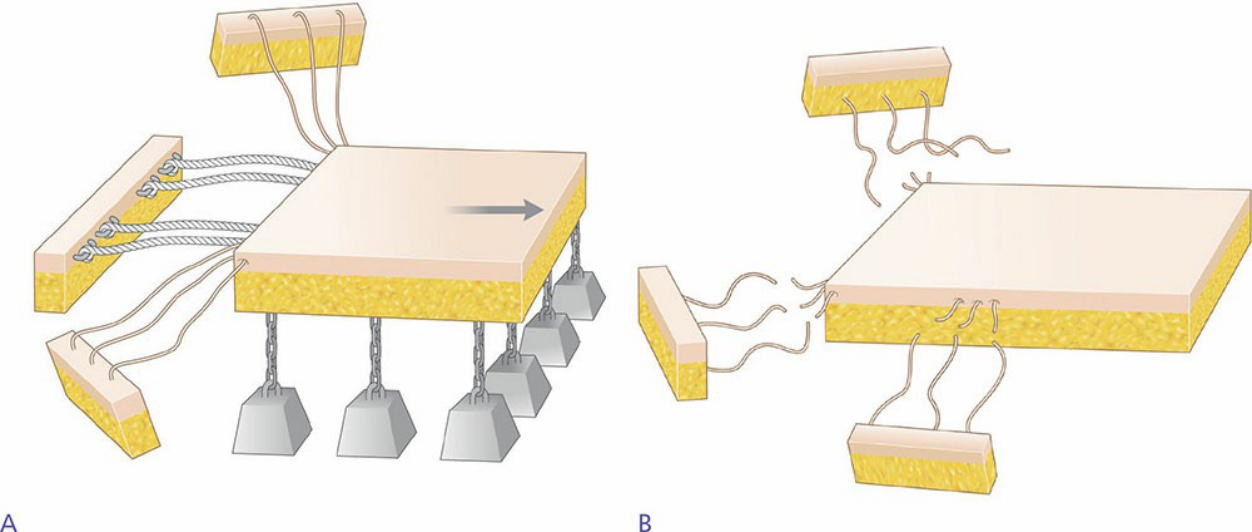
Figure 20-5. (A) Prior to the incision of an advancement flap, the surrounding skin creates horizontal restraint. (B) Undermining a flap removes deep restraint, which is secondary to the flap’s connections to underlying deep structures.
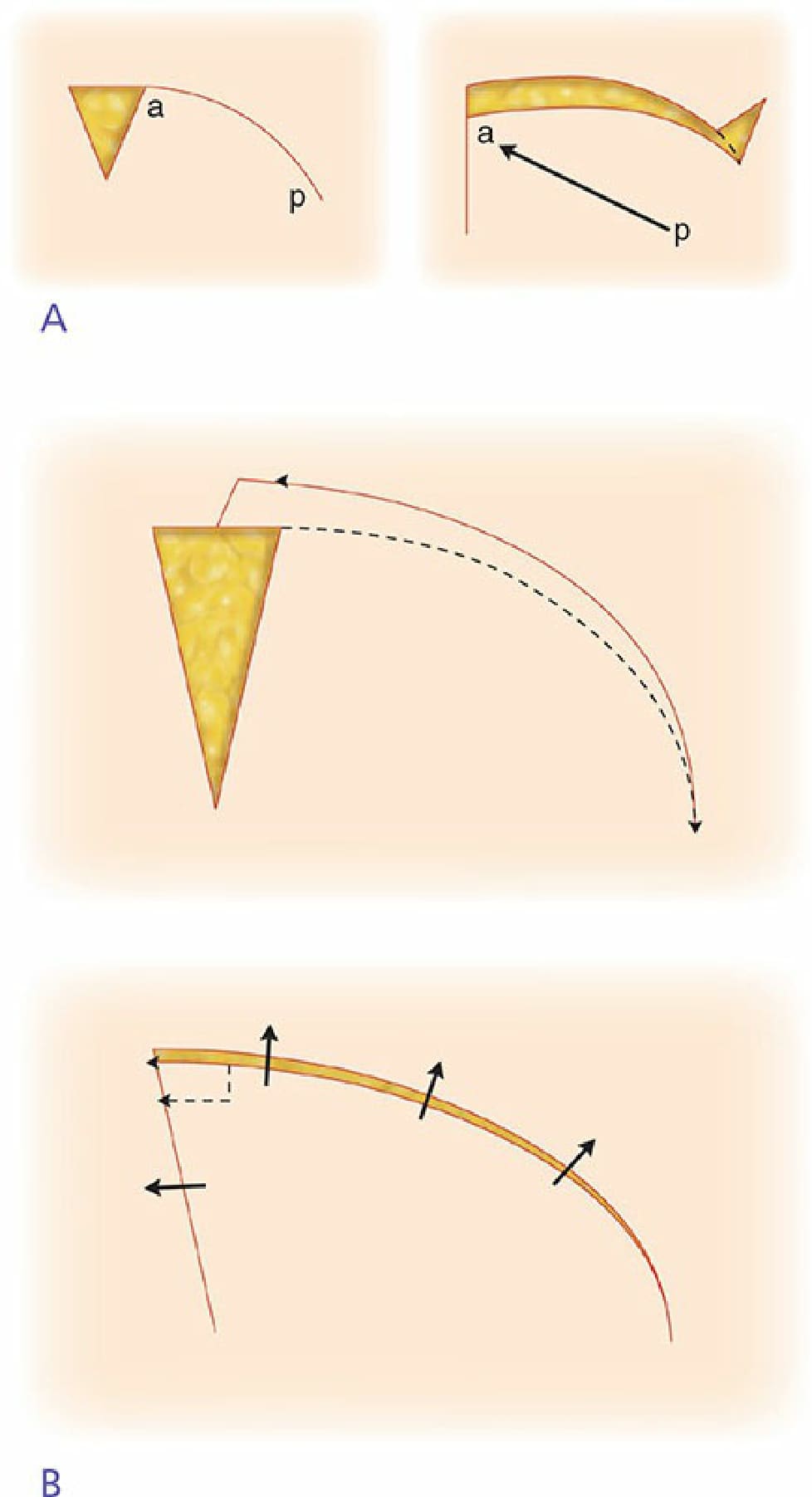
Figure 20-6. (A) A rotation flap is planned. The rotational movement of the flap creates a focus of pivotal restraint or rotational shortening. This limits the primary movement of the flap and the planned flap does not completely fill the primary defect. (B) One can compensate for pivotal restraint by extending the leading edge of a rotation flap. This allows for full closure of the primary defect without unnecessary tension.
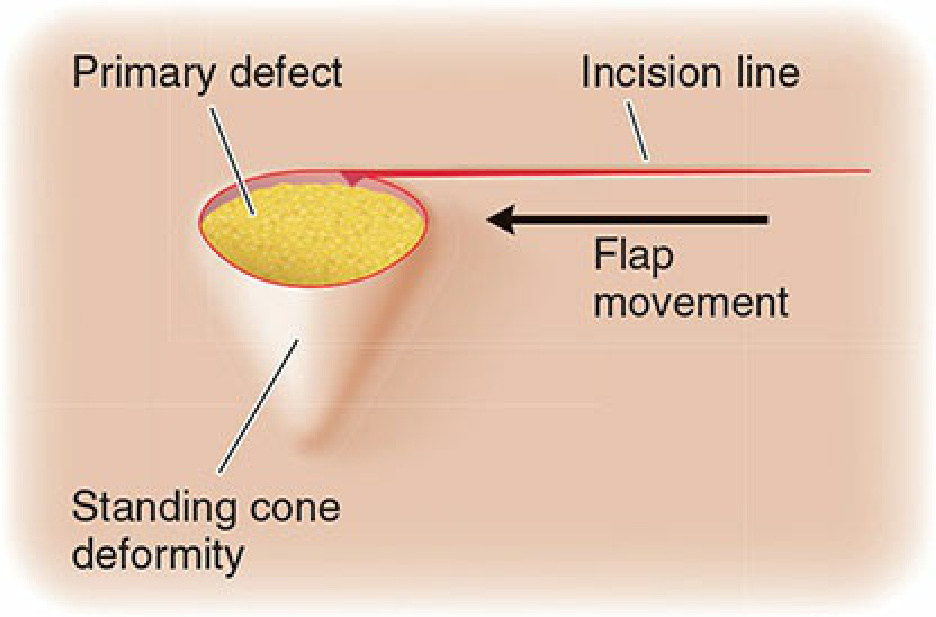
Figure 20-7. Compression of a standing cone deformity or dog ear provides a focus of obstructive restraint against primary flap movement as the extra tissue functions as a physical barrier impeding the desired primary movement.