Marking
Marking
Skin marking is important when preparing for linear closures; many surgeons draw a fusiform (or rhombus) shape to delineate the planned excision. Another approach that minimizes the amount of tissue marking used is to draw only minimal markings that outline the closure vector, closure extent, and margins around the lesion to be excised (Fig. 18-8).
Regardless of the planned defect shape, it may be useful to mark additional anatomic landmarks as well. On the face, cosmetic subunit boundaries may be marked prior to local anesthetic infiltration (Fig. 18-9). On the extremities, particularly when more than one vector appears a priori appropriate, both vectors may be drawn out and prioritized
(Fig. 18-10). Finally, when working around tattoos or near large superficial vessels, pacemaker leads, or other structures that should be avoided, these may be marked as well in a clear and consistent manner (Fig. 18-11).
Most dermatologic surgeons use felt-tipped surgical marking pens given their ease of use and low cost; patients should be told that any residual ink may be removed with alcohol. Other options include gentian violet, specialized white tissue markers, and white eyeliner markers.

Figure 18-8. Minimal markings that outline the closure vector, closure extent, and margins around the lesion to be excised can be used. This provides key information to the assistant for local anesthesia infiltration while using a minimal amount of ink that may later need to be removed.
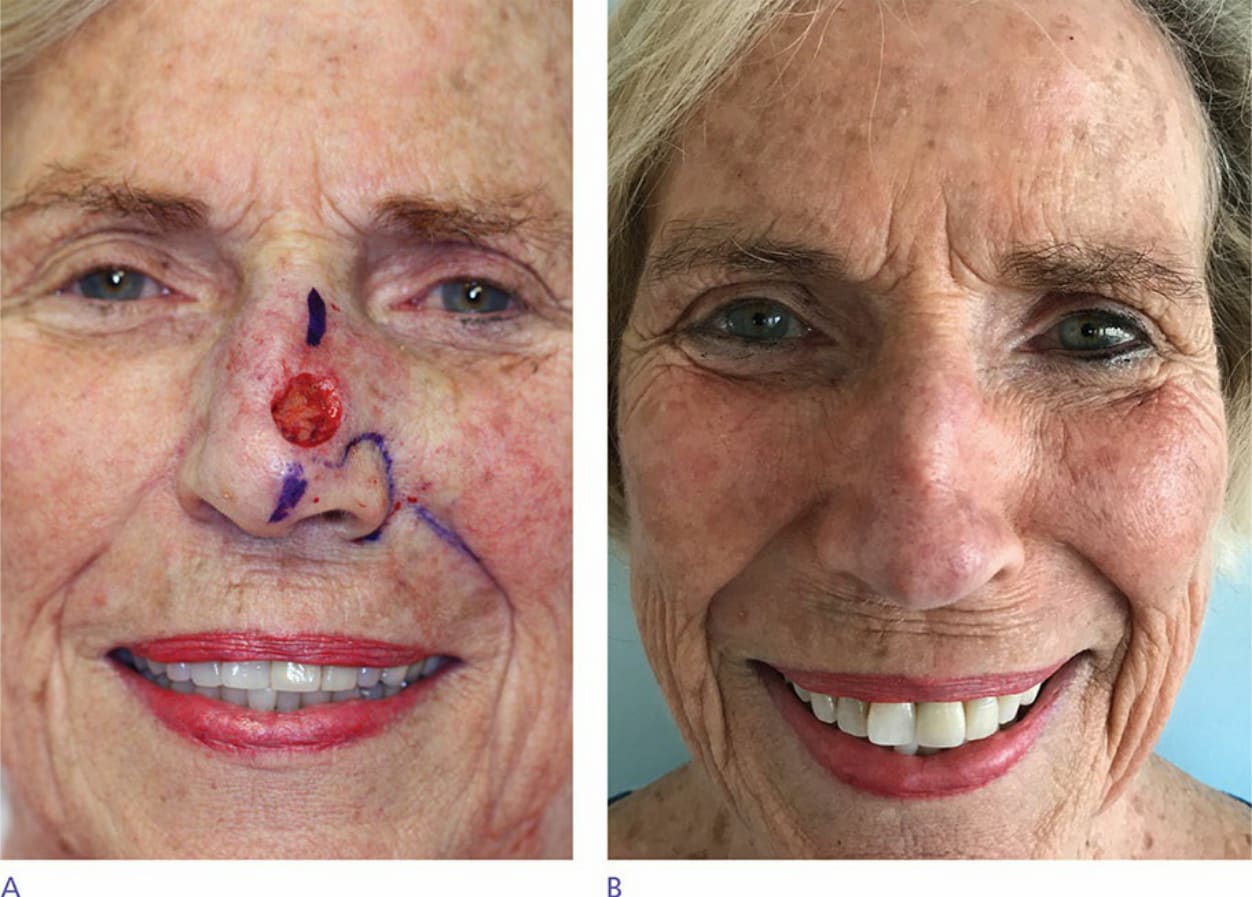
Figure 18-9. Cosmetic subunit boundaries may be marked prior to local anesthetic infiltration. A. Preoperative photograph. B. Postoperative photograph.

Figure 18-10. Multiple tension vectors may be drawn out if needed and sufficient local anesthetic may be infused to use either vector. A circular excision may be performed and the lowest tension vector can then be chosen.

Figure 18-11. Marking structures to be avoided in a clear manner is a helpful preoperative step.