Snip
Snip
A snip biopsy is performed by utilizing surgical scissors, such as gradle scissors, to remove a pedunculated lesion, generally at its base. After local anesthesia is obtained, care should be taken to avoid elevating the target of the biopsy with forceps, as a snip biopsy at the base of a manipulated pedunculated papule will result in a depressed postprocedure scar. Instead, the papule should be snipped at its base in the resting position, which should result in minimal postprocedure scarring.

Figure 14-5. The punch is twisted gently.

Figure 14-6. This continues until the entire device is inserted (when working on the trunk) or once the deep fat has been entered, as seen here.
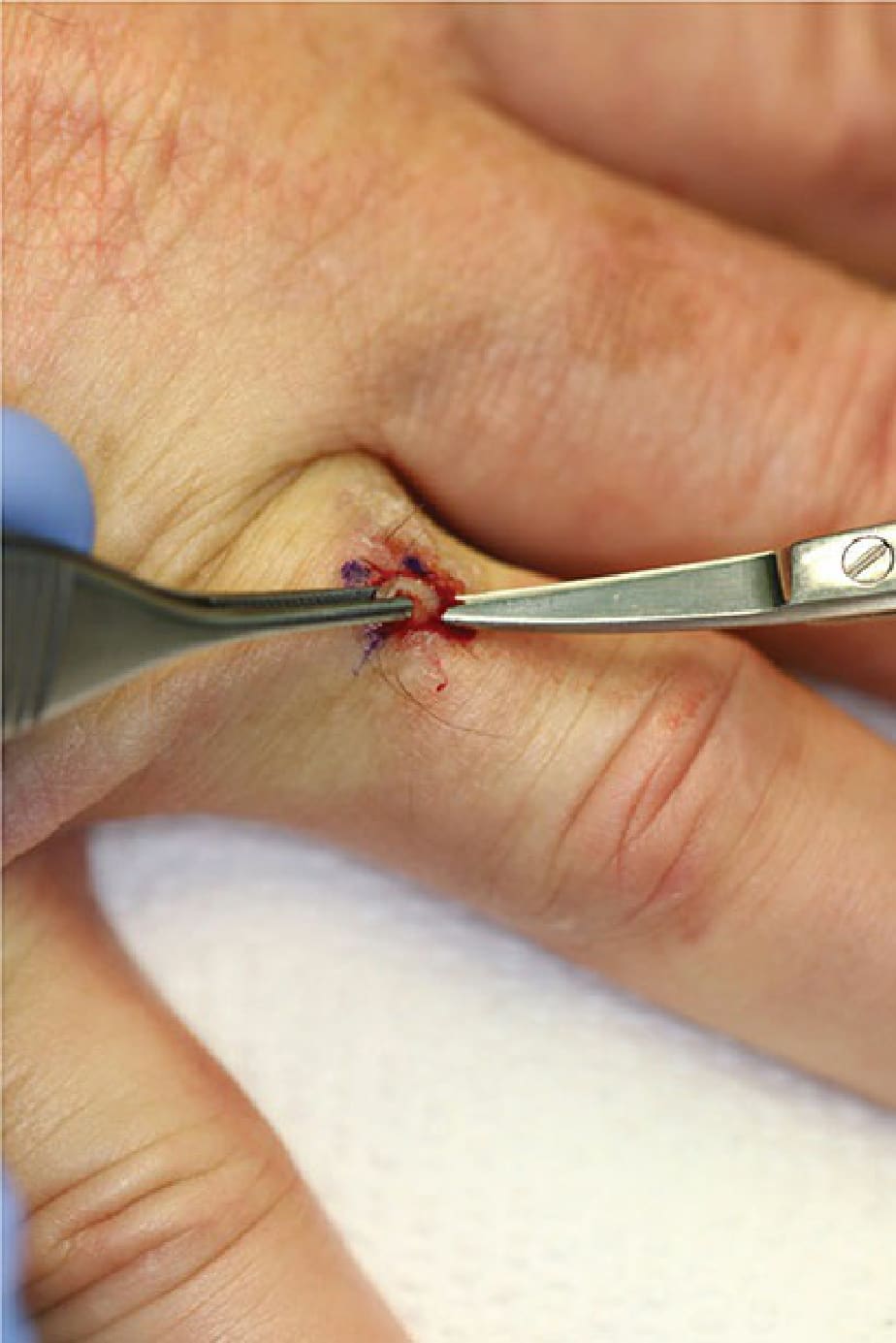
Figure 14-7. The specimen is grasped with forceps, elevated, and the base is snipped if needed at the level of the deep fat.

Figure 14-8. The resulting oval defect should be assessed for the ideal closure vector.

Figure 14-9. A suture is placed.

Figure 14-10. The cruciate mattress suture, essentially two throws of a simple running suture, is useful for punch biopsy closures.