Emergency equipment
Emergency equipment
Surgery limited to the skin and subcutaneous tissue, when performed under local anesthesia, does not require the need for emergency equipment and continues to be exempted by most state regulations. It remains the responsibility of the physician to ensure that the surgical facility is in compliance with local and state government regulatory bodies.
More advanced surgical suites should be equipped with an emergency crash cart in case of cardiopulmonary arrest or life-threatening drug reaction. Key office staff should be trained in basic CPR and ACLS. In addition, an emergency plan for patient transfer to a hospital should be in place.
As a general guideline, an emergency crash cart should include the following: automated external defibrillator (AED), oropharyngeal airway, laryngoscope with endotracheal tubes of various sizes, positive-pressure ventilation device with airways of various types and sizes, oxygen tank with delivery system, IV catheters of various sizes, bags of intravenous fluids, prefilled syringes/ampules including epinephrine, atropine, dextrose, lidocaine, sodium bicarbonate, hydrocortisone, naloxone,
flumazenil, diphenhydramine, and furosemide (Table 4-3).
Other emergency items recommended for the surgical suite include blood pressure/pulse monitoring, a pulse oximeter, a suction device, fire extinguisher, and eyewash station.
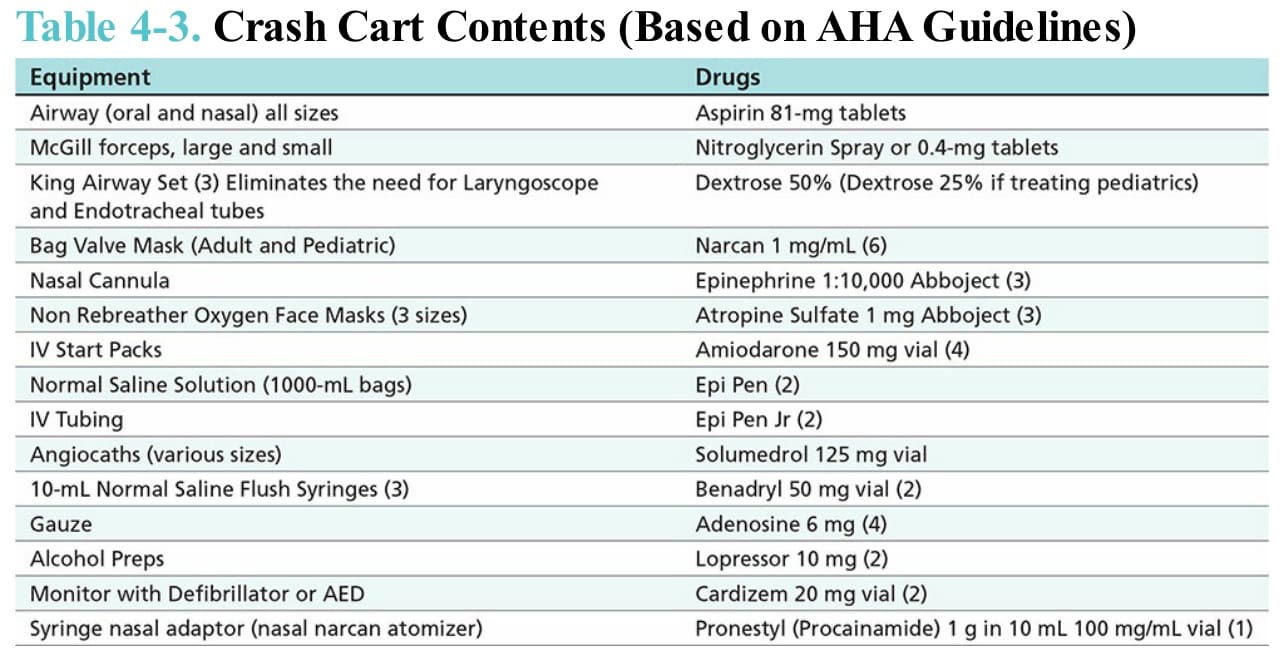
Table 4-3. Crash Cart Contents (Based on AHA Guidelines)